

Cardiovascular toxicity profiles of immune checkpoint inhibitors with or without angiogenesis inhibitors: a real-world pharmacovigilance analysis based on the FAERS database from 2014 to 2022
- PMID: 37292205
- PMCID: PMC10244526
- DOI: 10.3389/fimmu.2023.1127128
Cardiovascular toxicity profiles of immune checkpoint inhibitors with or without angiogenesis inhibitors: a real-world pharmacovigilance analysis based on the FAERS database from 2014 to 2022
Abstract
Background: Immune checkpoint inhibitors (ICIs) combined with angiogenesis inhibitors (AGIs) have become increasingly available for multiple types of cancers, although the cardiovascular safety profiles of this combination therapy in real-world settings have not been elucidated to date. Therefore, we aimed to comprehensively investigate the cardiovascular toxicity profiles of ICIs combined with AGIs in comparison with ICIs alone.
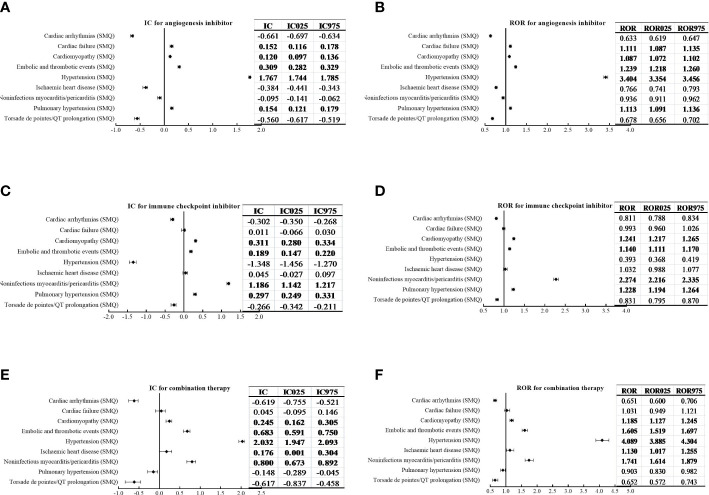
Methods: The Food and Drug Administration Adverse Event Reporting System (FAERS) database from the 1st quarter of 2014 to the 1st quarter of 2022 was retrospectively queried to extract reports of cardiovascular adverse events (AEs) associated with ICIs alone, AGIs alone and combination therapy. To perform disproportionality analysis, the reporting odds ratios (RORs) and information components (ICs) were calculated with statistical shrinkage transformation formulas and a lower limit of the 95% confidence interval (CI) for ROR (ROR025) > 1 or IC (IC025) > 0 with at least 3 reports was considered statistically significant.
Results: A total of 18 854 cardiovascular AE cases/26 059 reports for ICIs alone, 47 168 cases/67 595 reports for AGIs alone, and 3 978 cases/5 263 reports for combination therapy were extracted. Compared to the entire database of patients without AGIs or ICIs, cardiovascular AEs were overreported in patients with combination therapy (IC025/ROR025 = 0.559/1.478), showing stronger signal strength than those taking ICIs alone (IC025/ROR025 = 0.118/1.086) or AGIs alone (IC025/ROR025 = 0.323/1.252). Importantly, compared with ICIs alone, combination therapy showed a decrease in signal strength for noninfectious myocarditis/pericarditis (IC025/ROR025 = 1.142/2.216 vs. IC025/ROR025 = 0.673/1.614), while an increase in signal value for embolic and thrombotic events (IC025/ROR025 = 0.147/1.111 vs. IC025/ROR025 = 0.591/1.519). For outcomes of cardiovascular AEs, the frequency of death and life-threatening AEs was lower for combination therapy than ICIs alone in noninfectious myocarditis/pericarditis (37.7% vs. 49.2%) as well as in embolic and thrombotic events (29.9% vs. 39.6%). Analysis among indications of cancer showed similar findings.
Conclusion: Overall, ICIs combined with AGIs showed a greater risk of cardiovascular AEs than ICIs alone, mainly due to an increase in embolic and thrombotic events while a decrease in noninfectious myocarditis/pericarditis. In addition, compared with ICIs alone, combination therapy presented a lower frequency of death and life-threatening in noninfectious myocarditis/pericarditis and embolic and thrombotic events.
Keywords: FAERS database; angiogenesis inhibitor; cardiovascular toxicity; combination therapy; disproportionality analysis; immune checkpoint inhibitor.
Copyright © 2023 Wang, Cui, Deng, Wang and Ren.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Immune-related adverse events of immune checkpoint inhibitors combined with angiogenesis inhibitors: A real-world pharmacovigilance analysis of the FDA Adverse Event Reporting System (FAERS) database (2014-2022).Int Immunopharmacol. 2024 Jul 30;136:112301. doi: 10.1016/j.intimp.2024.112301. Epub 2024 Jun 4. Int Immunopharmacol. 2024. PMID: 38838553
-
Cardiovascular toxicity associated with angiogenesis inhibitors: A comprehensive pharmacovigilance analysis based on the FDA Adverse Event Reporting System database from 2014 to 2021.Front Cardiovasc Med. 2022 Oct 13;9:988013. doi: 10.3389/fcvm.2022.988013. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312283 Free PMC article.
-
Hepatic failure associated with immune checkpoint inhibitors: An analysis of the Food and Drug Administration Adverse Event Reporting System database.Cancer Med. 2023 Apr;12(8):9167-9174. doi: 10.1002/cam4.5655. Epub 2023 Feb 3. Cancer Med. 2023. PMID: 36734333 Free PMC article.
-
Acute kidney injury associated with immune checkpoint inhibitors: A pharmacovigilance study.Int Immunopharmacol. 2022 Dec;113(Pt A):109350. doi: 10.1016/j.intimp.2022.109350. Epub 2022 Oct 20. Int Immunopharmacol. 2022. PMID: 36272360
-
Allograft rejection following immune checkpoint inhibitors in solid organ transplant recipients: A safety analysis from a literature review and a pharmacovigilance system.Cancer Med. 2023 Mar;12(5):5181-5194. doi: 10.1002/cam4.5394. Epub 2022 Dec 12. Cancer Med. 2023. PMID: 36504294 Free PMC article. Review.
Cited by
-
Toxicity in combined therapies for tumours treatments: a lesson from BAG3 in the TME?Front Immunol. 2023 Jul 20;14:1241543. doi: 10.3389/fimmu.2023.1241543. eCollection 2023. Front Immunol. 2023. PMID: 37554328 Free PMC article. No abstract available.
-
Adverse reactions of immune checkpoint inhibitors combined with angiogenesis inhibitors: A pharmacovigilance analysis of drug-drug interactions.Int J Immunopathol Pharmacol. 2024 Jan-Dec;38:3946320241305390. doi: 10.1177/03946320241305390. Int J Immunopathol Pharmacol. 2024. PMID: 39660594 Free PMC article.
-
Medication overdose data analysis: a review of medication error reports in the FDA adverse event reporting system (FAERS).BMC Pharmacol Toxicol. 2023 Aug 4;24(1):41. doi: 10.1186/s40360-023-00681-y. BMC Pharmacol Toxicol. 2023. PMID: 37542326 Free PMC article. Review.
-
Postmarket safety profile of suicide/self-injury for GLP-1 receptor agonist: a real-world pharmacovigilance analysis.Eur Psychiatry. 2023 Nov 30;66(1):e99. doi: 10.1192/j.eurpsy.2023.2474. Eur Psychiatry. 2023. PMID: 38031404 Free PMC article.
-
Targeting the Renin-angiotensin-aldosterone System (RAAS) for Cardiovascular Protection and Enhanced Oncological Outcomes: Review.Curr Treat Options Oncol. 2024 Nov;25(11):1406-1427. doi: 10.1007/s11864-024-01270-9. Epub 2024 Oct 18. Curr Treat Options Oncol. 2024. PMID: 39422794 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical