

Case Report: Persistent response to combination therapy of pemigatinib, chemotherapy, and immune checkpoint inhibitor in a patient with advanced intrahepatic cholangiocarcinoma
- PMID: 37292215
- PMCID: PMC10245386
- DOI: 10.3389/fimmu.2023.1124482
Case Report: Persistent response to combination therapy of pemigatinib, chemotherapy, and immune checkpoint inhibitor in a patient with advanced intrahepatic cholangiocarcinoma
Abstract
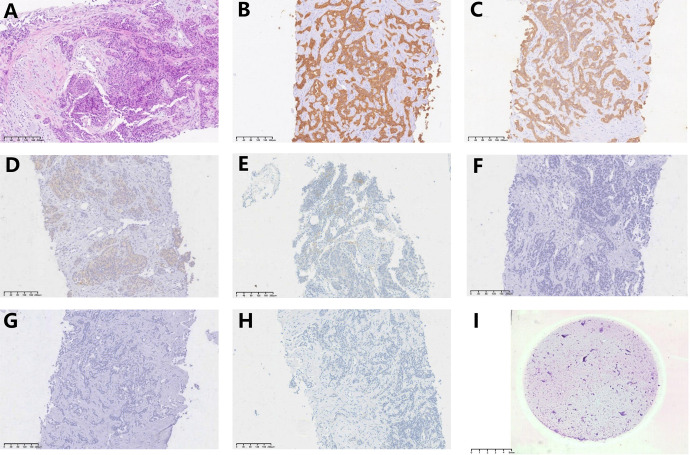
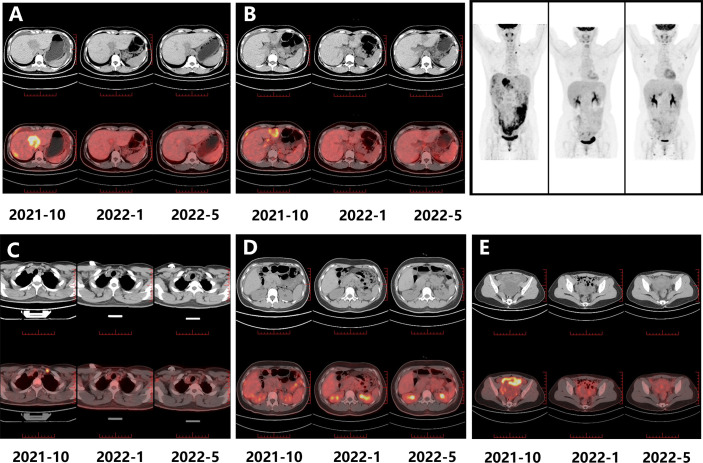
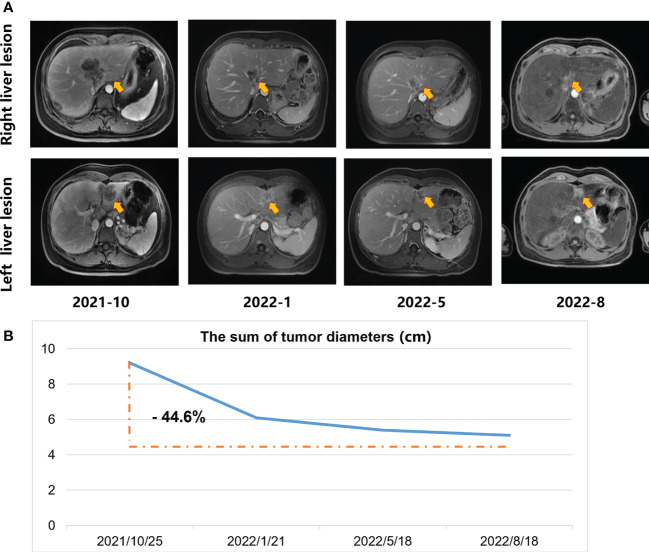
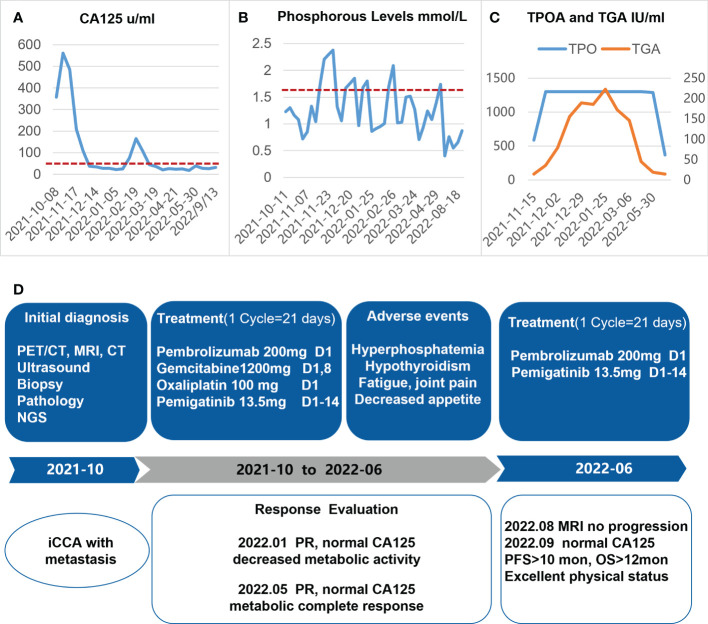
Patients with advanced intrahepatic cholangiocarcinoma (iCCA) often have a poor prognosis. Recent advancements in targeted molecular therapy and immunotherapy have been made. Herein, we report a case of advanced iCCA treated with a combination of pemigatinib (a selective FGFR inhibitor), chemotherapy, and an immune checkpoint inhibitor. A 34-year-old female was diagnosed with advanced iCCA with multiple liver masses and metastases in the peritoneum and lymph nodes. Next-generation sequencing (NGS) identified the genetic mutations. An FGFR2-BICC1 gene fusion was found in this patient. The patient was treated with pemigatinib in combination with pembrolizumab plus systemic gemcitabine and oxaliplatin. After 9 cycles of the combination therapy, the patient achieved a partial response, complete metabolic response, and normalization of tumor markers. Sequentially, the patient received pemigatinib and pembrolizumab for 3 months. Due to the elevated tumor biomarker, she is currently receiving chemotherapy, pemigatinib, and pembrolizumab treatment again. She regained an excellent physical status after 16 months of treatment. To the best of our knowledge, this was the first reported case of advanced iCCA successfully treated with a combination of pemigatinib, chemotherapy, and ICIs as a first-line regimen. This treatment combination may be effective and safe in the advanced iCCA.
Keywords: FGFR inhibitors; advanced intrahepatic cholangiocarcinoma; combined therapy; immune checkpoint inhibitor; pemigatinib.
Copyright © 2023 Zhang, Wang, Du, Zhao, Pan, Zhang, Wang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Persistent response to combination therapy of pemigatinib and chemotherapy in a child of combined hepatocellular-cholangiocarcinoma with FGFR2 fusion.Mol Cancer. 2024 Dec 6;23(1):269. doi: 10.1186/s12943-024-02190-w. Mol Cancer. 2024. PMID: 39643892 Free PMC article.
-
Pemigatinib: A Review in Advanced Cholangiocarcinoma.Target Oncol. 2024 Jan;19(1):107-114. doi: 10.1007/s11523-023-01024-x. Epub 2024 Jan 11. Target Oncol. 2024. PMID: 38206555 Review.
-
Treating intrahepatic cholangiocarcinoma with pemigatinib: two case reports of Nordic patients.Acta Oncol. 2025 Apr 15;64:534-539. doi: 10.2340/1651-226X.2025.42073. Acta Oncol. 2025. PMID: 40230323 Free PMC article.
-
Pemigatinib combined with immunotherapy and stereotactic body radiation therapy for FGFR2 fusion-positive advanced intrahepatic cholangiocarcinoma with brain metastasis: a Case Report.Front Pharmacol. 2024 Dec 4;15:1509891. doi: 10.3389/fphar.2024.1509891. eCollection 2024. Front Pharmacol. 2024. PMID: 39697545 Free PMC article.
-
Targeting FGFR in intrahepatic cholangiocarcinoma [iCCA]: leading the way for precision medicine in biliary tract cancer [BTC]?Expert Opin Investig Drugs. 2021 Apr;30(4):463-477. doi: 10.1080/13543784.2021.1900821. Epub 2021 Apr 11. Expert Opin Investig Drugs. 2021. PMID: 33678096 Review.
Cited by
-
First Successful Treatment of Advanced Intrahepatic Cholangiocarcinoma with Tasurgratinib Following Regulatory Approval: A Case Report from Clinical Practice.Int J Mol Sci. 2025 Jun 11;26(12):5586. doi: 10.3390/ijms26125586. Int J Mol Sci. 2025. PMID: 40565050 Free PMC article.
-
Case report: Translational treatment of unresectable intrahepatic cholangiocarcinoma: Tislelizumab, Lenvatinib, and GEMOX in one case.Front Oncol. 2024 Jul 15;14:1428370. doi: 10.3389/fonc.2024.1428370. eCollection 2024. Front Oncol. 2024. PMID: 39077469 Free PMC article.
-
Evolving approaches in advanced gallbladder cancer with complete pathological response using chemo‑immunotherapy: A case report.Oncol Lett. 2024 Aug 2;28(4):473. doi: 10.3892/ol.2024.14606. eCollection 2024 Oct. Oncol Lett. 2024. PMID: 39161332 Free PMC article.
-
Programmed Cell Death Pathways in Cholangiocarcinoma: Opportunities for Targeted Therapy.Cancers (Basel). 2023 Jul 15;15(14):3638. doi: 10.3390/cancers15143638. Cancers (Basel). 2023. PMID: 37509299 Free PMC article. Review.
References
-
- Ruzzenente A, Conci S, Valdegamberi A, Pedrazzani C, Guglielmi A. Role of surgery in the treatment of intrahepatic cholangiocarcinoma. Eur Rev Med Pharmacol Sci (2015) 19:2892–900. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous