

This is a preprint.
Insights from rare variants into the genetic architecture and biology of youth-onset type 2 diabetes
- PMID: 37292813
- PMCID: PMC10246295
- DOI: 10.21203/rs.3.rs-2886343/v1
Insights from rare variants into the genetic architecture and biology of youth-onset type 2 diabetes
Update in
-
Genetic architecture and biology of youth-onset type 2 diabetes.Nat Metab. 2024 Feb;6(2):226-237. doi: 10.1038/s42255-023-00970-0. Epub 2024 Jan 26. Nat Metab. 2024. PMID: 38278947 Free PMC article.
Abstract
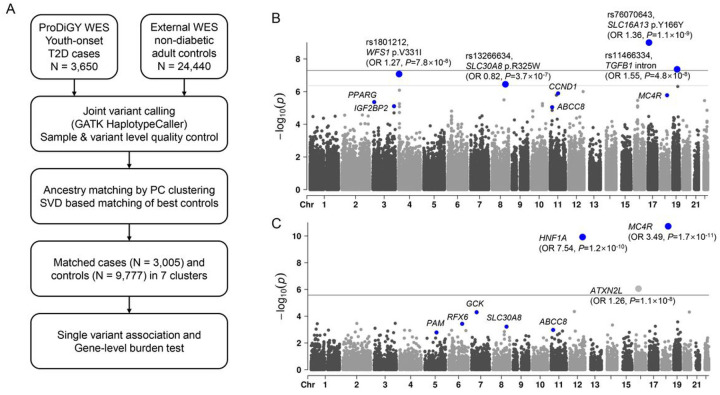
Youth-onset type 2 diabetes (T2D) is a growing public health concern. Its genetic basis and relationship to other forms of diabetes are largely unknown. To gain insight into the genetic architecture and biology of youth-onset T2D, we analyzed exome sequences of 3,005 youth-onset T2D cases and 9,777 ancestry matched adult controls. We identified (a) monogenic diabetes variants in 2.1% of individuals; (b) two exome-wide significant (P < 4.3×10-7) common coding variant associations (in WFS1 and SLC30A8); (c) three exome-wide significant (P < 2.5×10-6) rare variant gene-level associations (HNF1A, MC4R, ATX2NL); and (d) rare variant association enrichments within 25 gene sets broadly related to obesity, monogenic diabetes, and β-cell function. Many association signals were shared between youth-onset and adult-onset T2D but had larger effects for youth-onset T2D risk (1.18-fold increase for common variants and 2.86-fold increase for rare variants). Both common and rare variant associations contributed more to youth-onset T2D liability variance than they did to adult-onset T2D, but the relative increase was larger for rare variant associations (5.0-fold) than for common variant associations (3.4-fold). Youth-onset T2D cases showed phenotypic differences depending on whether their genetic risk was driven by common variants (primarily related to insulin resistance) or rare variants (primarily related to β-cell dysfunction). These data paint a picture of youth-onset T2D as a disease genetically similar to both monogenic diabetes and adult-onset T2D, in which genetic heterogeneity might be used to sub-classify patients for different treatment strategies.
Conflict of interest statement
CONFLICT OF INTEREST J.C.F. has received speaking honoraria from AstraZeneca and Novo Nordisk for scientific talks over which he had full control of content; his wife has received a consulting honorarium from Novartis. The remaining authors declare no competing interests relevant to this study.
Figures



References
Publication types
Grants and funding
- R01 DK078616/DK/NIDDK NIH HHS/United States
- UC4 DK108173/DK/NIDDK NIH HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- U01 DP000244/DP/NCCDPHP CDC HHS/United States
- P30 DK036836/DK/NIDDK NIH HHS/United States
- M01 RR014467/RR/NCRR NIH HHS/United States
- U01 DK085526/DK/NIDDK NIH HHS/United States
- U01 DK105554/DK/NIDDK NIH HHS/United States
- U18 DP002708/DP/NCCDPHP CDC HHS/United States
- R01 DK125490/DK/NIDDK NIH HHS/United States
- U01 DK061254/DK/NIDDK NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- P30 DK057516/DK/NIDDK NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- U18 DP006131/DP/NCCDPHP CDC HHS/United States
- U01 DP000247/DP/NCCDPHP CDC HHS/United States
- U54 HG003067/HG/NHGRI NIH HHS/United States
- U18 DP002710/DP/NCCDPHP CDC HHS/United States
- K23 DK120932/DK/NIDDK NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- U18 DP006134/DP/NCCDPHP CDC HHS/United States
- U18 DP006138/DP/NCCDPHP CDC HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- UL1 TR000154/TR/NCATS NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- U18 DP002714/DP/NCCDPHP CDC HHS/United States
- U01 DK061242/DK/NIDDK NIH HHS/United States
- U01 DP000248/DP/NCCDPHP CDC HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- UL1 TR000062/TR/NCATS NIH HHS/United States
- R01 AG008122/AG/NIA NIH HHS/United States
- U01 DK061212/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- R01 AG033193/AG/NIA NIH HHS/United States
- U01 DK061230/DK/NIDDK NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- U18 DP006136/DP/NCCDPHP CDC HHS/United States
- U18 DP002709/DP/NCCDPHP CDC HHS/United States
- U18 DP006133/DP/NCCDPHP CDC HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- UM1 TR004528/TR/NCATS NIH HHS/United States
- U18 DP006139/DP/NCCDPHP CDC HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- M01 RR000084/RR/NCRR NIH HHS/United States
- U01 DP000250/DP/NCCDPHP CDC HHS/United States
- K24 HL157960/HL/NHLBI NIH HHS/United States
- U01 DP000246/DP/NCCDPHP CDC HHS/United States
- UL1 TR001450/TR/NCATS NIH HHS/United States
- U01 DP000254/DP/NCCDPHP CDC HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U01 DK061239/DK/NIDDK NIH HHS/United States
- HIR 10-001/HX/HSRD VA/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
