

This is a preprint.
Lipidomics for diagnosis and prognosis of pulmonary hypertension
- PMID: 37292870
- PMCID: PMC10246148
- DOI: 10.1101/2023.05.17.23289772
Lipidomics for diagnosis and prognosis of pulmonary hypertension
Update in
-
Lipid Ratios for Diagnosis and Prognosis of Pulmonary Hypertension.Am J Respir Crit Care Med. 2025 Jul;211(7):1264-1276. doi: 10.1164/rccm.202407-1345OC. Am J Respir Crit Care Med. 2025. PMID: 40343938 Free PMC article.
Abstract
Background: Pulmonary hypertension (PH) poses a significant health threat with high morbidity and mortality, necessitating improved diagnostic tools for enhanced management. Current biomarkers for PH lack functionality and comprehensive diagnostic and prognostic capabilities. Therefore, there is a critical need to develop biomarkers that address these gaps in PH diagnostics and prognosis.
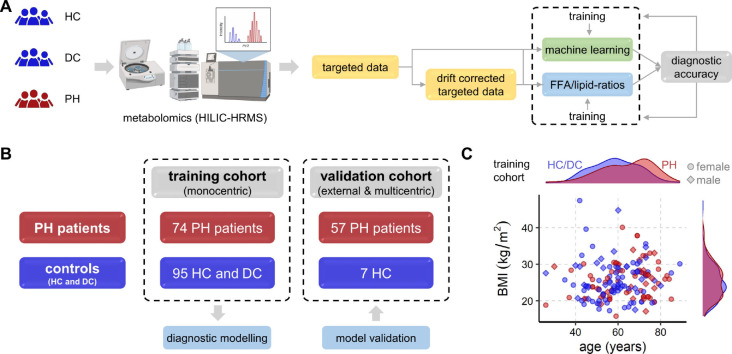
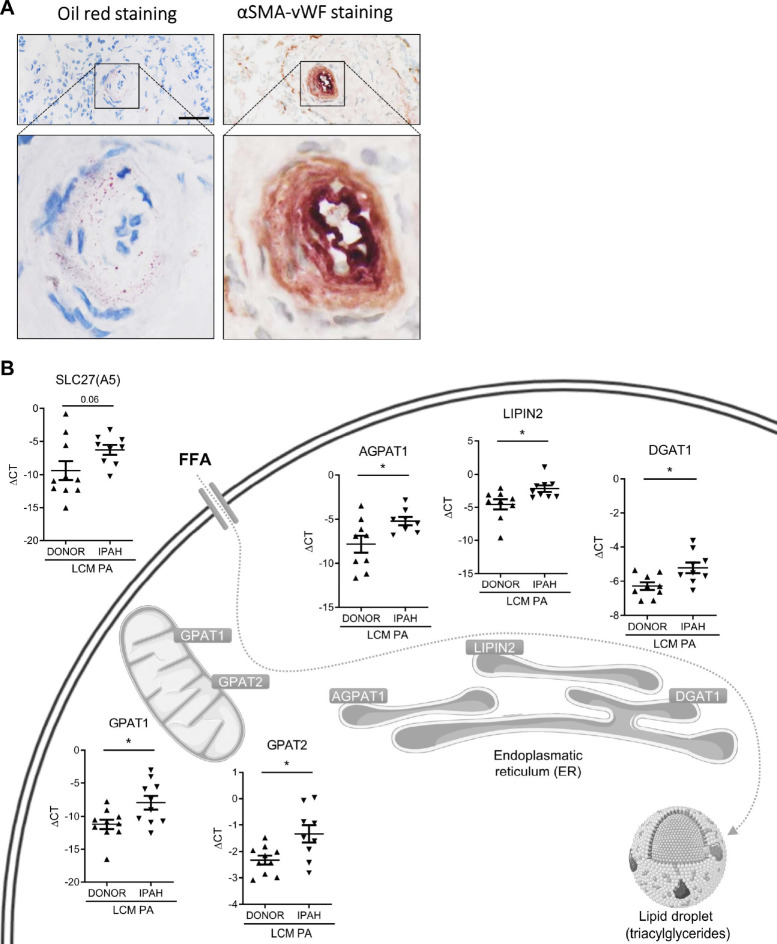
Methods: To address this need, we employed a comprehensive metabolomics analysis in 233 blood based samples coupled with machine learning analysis. For functional insights, human pulmonary arteries (PA) of idiopathic pulmonary arterial hypertension (PAH) lungs were investigated and the effect of extrinsic FFAs on human PA endothelial and smooth muscle cells was tested in vitro.
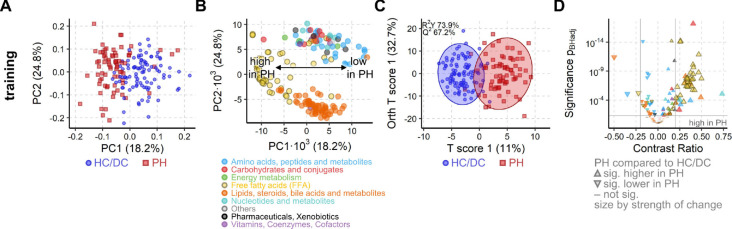
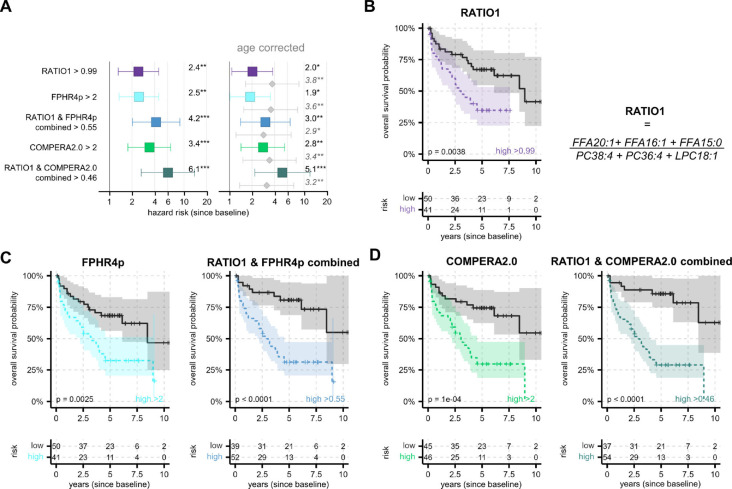
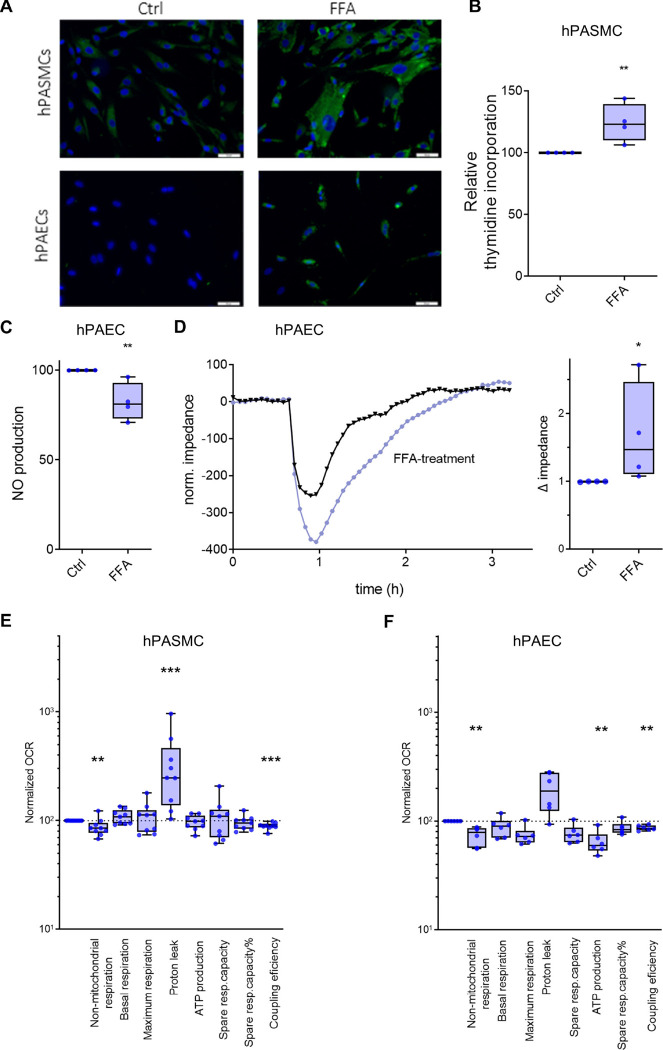
Results: PA of idiopathic PAH lungs showed lipid accumulation and altered expression of lipid homeostasis-related genes. In PA smooth muscle cells, extrinsic FFAs caused excessive proliferation and endothelial barrier dysfunction in PA endothelial cells, both hallmarks of PAH.In the training cohort of 74 PH patients, 30 disease controls without PH, and 65 healthy controls, diagnostic and prognostic markers were identified and subsequently validated in an independent cohort. Exploratory analysis showed a highly impacted metabolome in PH patients and machine learning confirmed a high diagnostic potential. Fully explainable specific free fatty acid (FFA)/lipid-ratios were derived, providing exceptional diagnostic accuracy with an area under the curve (AUC) of 0.89 in the training and 0.90 in the validation cohort, outperforming machine learning results. These ratios were also prognostic and complemented established clinical prognostic PAH scores (FPHR4p and COMPERA2.0), significantly increasing their hazard ratios (HR) from 2.5 and 3.4 to 4.2 and 6.1, respectively.
Conclusion: In conclusion, our research confirms the significance of lipidomic alterations in PH, introducing innovative diagnostic and prognostic biomarkers. These findings may have the potential to reshape PH management strategies.
Keywords: biomarker; blood-based test; fatty acid to lipid ratio; lipidomics; prognosis; pulmonary hypertension.
Conflict of interest statement
Competing interests Several authors (NB, CM, AO, BMN, HO) are inventors of the patent “Biomarker for the diagnosis of pulmonary hypertension (PH)” WO2017153472A1 (priority date 09.03.2016, granted in US, KR, JP, pending in CA, EP, AU) being jointly held by CBmed Gmbh, Joanneum Research Forschungsgesellschaft mbH, Medical University Graz and Ludwig Boltzmann Gesellschaft GmbH. The authors received no personal financial gain from the patent. During work on this publication NB was partially employed at CBmed GmbH. TP is chief scientific officer (CSO) of CBmed GmbH. EZ and CM were employed at Joanneum Research Forschungsgesellschaft mbH. The employing companies provided support in the form of salaries, materials and reagents but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. VF received honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen, Chiesi, BMS, and Boehringer Ingelheim and support for attending meetings, and/or travel from Janssen, MSD, and Boehringer Ingelheim outside the submitted work. CN received support for attending meetings, and/or travel from Boehringer Ingelheim and Inventiva pharma outside the submitted work. BAM reports personal fees from Actelion Pharmaceuticals, Tenax and Regeneron, grants from Deerfield Company, NIH (5R01HL139613-03, R01HL163960, R01HL153502, R01HL155096-01), Boston Biomedical Innovation Center (BBIC), Brigham IGNITE award, Cardiovascular Medical research Education Foundation outside the submitted work. BAM reports patent PCT/US2019/059890 (pending), PCT/US2020/066886 (pending) and #9,605,047 (granted) not licensed and outside the submitted work. SU received grants from the Swiss National Science Foundation, Zürich and Swiss Lung League, EMDO-Foundation, Orpha-Swiss, Janssen and MSD all unrelated to the present work. SU received consultancy fees and travel support from Orpha-Swiss, Janssen, MSD and Novartis unrelated to the present work. TJL reports grants for his institution from Acceleron Pharma, Gossamer Bio, Janssen-Cilag, and United Therapeutics; personal fees and non-financial support from Acceleron Pharma, AstraZeneca, Boehringer Ingelheim, Gossamer Bio, Ferrer, Janssen-Cilag, MSD, Orphacare, and Pfizer outside the submitted work. KH is a consultant at Medtronic Österreich GmbH outside the submitted work. TP reports grants from AstraZeneca, Novo Nordisk, Sanofi paid to the Medical University of Graz outside the submitted work. TP reports personal fees and nonfinancial support from Novo Nordisk and Roche Diagnostics outside the submitted work. HO reports grants from Bayer, Unither, Actelion, Roche, Boehringer Ingelheim, and Pfizer. HO reports personal fees and non-financial support from Medupdate and Mondial, AOP, Astra Zeneca, Bayer, Boehringer Ingelheim, Chiesi, Ferrer, Menarini, MSD, and GSK, Iqvia, Janssen, Novartis, and Pfizer outside the submitted work. AO received honoraria for presentations and support for attending meetings, and/or travel from MSD outside the submitted work. No conflict of interest, financial or otherwise, are declared by the authors HL and UB.
Figures

References
-
- Hoeper MM, Humbert M, Souza R, et al. A global view of pulmonary hypertension. Lancet Respir Med 2016; 4: 306–322. - PubMed
-
- Vachiéry J-L, Tedford RJ, Rosenkranz S, et al. Pulmonary hypertension due to left heart disease. European Respiratory Journal 2019; 53: 1801897.
Online References
-
- Kovacs G, Avian A, Bachmaier G, et al. Severe Pulmonary Hypertension in COPD: Impact on Survival and Diagnostic Approach. Chest 2022; 162: 202–212. - PubMed
-
- Galiè N, Humbert M, Vachiery J-L, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015; 46: 903–75. - PubMed
-
- Hoffmann J, Wilhelm J, Marsh LM, et al. Distinct differences in gene expression patterns in pulmonary arteries of patients with chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis with pulmonary hypertension. Am J Respir Crit Care Med 2014; 190: 98–111. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources