

This is a preprint.
A Standardized Antiviral Pipeline for Human Norovirus in Human Intestinal Enteroids Demonstrates No Antiviral Activity of Nitazoxanide
- PMID: 37293103
- PMCID: PMC10245936
- DOI: 10.1101/2023.05.23.542011
A Standardized Antiviral Pipeline for Human Norovirus in Human Intestinal Enteroids Demonstrates No Antiviral Activity of Nitazoxanide
Update in
-
Standardization of an antiviral pipeline for human norovirus in human intestinal enteroids demonstrates nitazoxanide has no to weak antiviral activity.Antimicrob Agents Chemother. 2023 Oct 18;67(10):e0063623. doi: 10.1128/aac.00636-23. Epub 2023 Oct 3. Antimicrob Agents Chemother. 2023. PMID: 37787556 Free PMC article.
Abstract
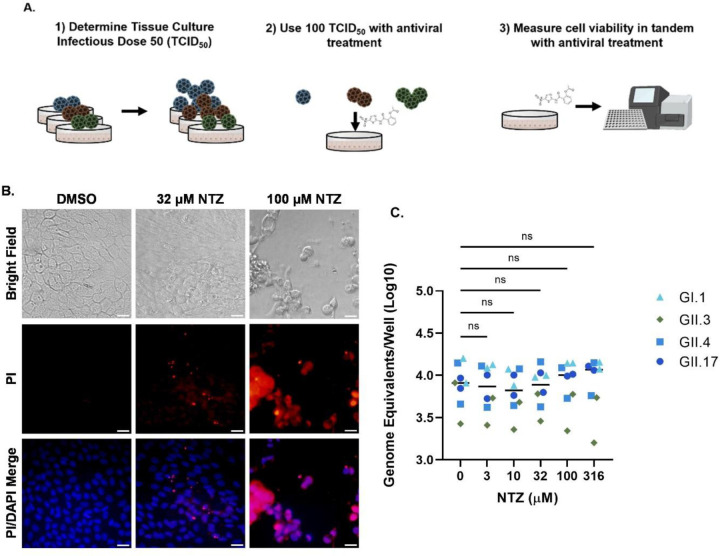
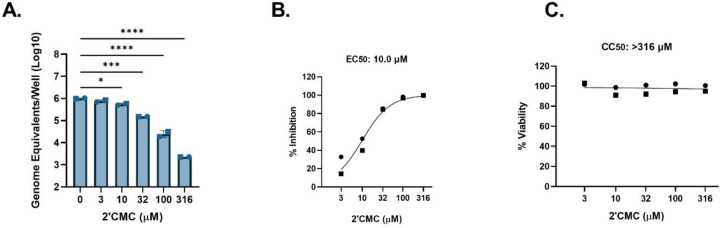
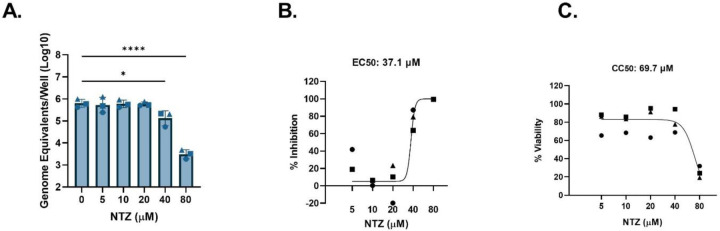
Human noroviruses (HuNoVs) are the leading cause of acute gastroenteritis. In immunocompetent hosts, symptoms usually resolve within three days; however, in immunocompromised persons, HuNoV infection can become persistent, debilitating, and sometimes life-threatening. There are no licensed therapeutics for HuNoV due to a near half-century delay in its cultivation. Treatment for chronic HuNoV infection in immunosuppressed patients anecdotally includes nitazoxanide, a broad-spectrum antimicrobial licensed for treatment of parasite-induced gastroenteritis. Despite its off-label use for chronic HuNoV infection, nitazoxanide has not been clearly demonstrated to be an effective treatment. In this study, we established a standardized pipeline for antiviral testing using multiple human small intestinal enteroid (HIE) lines representing different intestinal segments and evaluated whether nitazoxanide inhibits replication of 5 HuNoV strains in vitro . Nitazoxanide did not exhibit high selective antiviral activity against any HuNoV strains tested, indicating it is not an effective antiviral for norovirus infection. HIEs are further demonstrated as a model to serve as a pre-clinical platform to test antivirals against human noroviruses to treat gastrointestinal disease.
Conflict of interest statement
Disclosure of interests
M.K.E. is named as an inventor on patents related to cloning of the Norwalk virus genome and HuNoV cultivation and has received research funding from Takeda Vaccines Business Unit (Cambridge, MA, USA). R.L.A. is named as an inventor on patents related to HuNoV cultivation and has received research support from Takeda Vaccines Business Unit (Cambridge, MA, USA).
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources