

Factors associated with circulatory death after out-of-hospital cardiac arrest: a population-based cluster analysis
- PMID: 37294400
- PMCID: PMC10256665
- DOI: 10.1186/s13613-023-01143-8
Factors associated with circulatory death after out-of-hospital cardiac arrest: a population-based cluster analysis
Abstract
Background: Out-of-hospital cardiac arrest (OHCA) is a common cause of death. Early circulatory failure is the most common reason for death within the first 48 h. This study in intensive care unit (ICU) patients with OHCA was designed to identify and characterize clusters based on clinical features and to determine the frequency of death from refractory postresuscitation shock (RPRS) in each cluster.
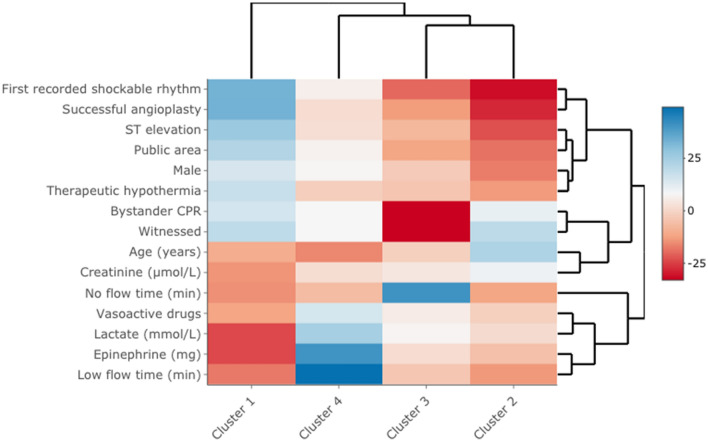
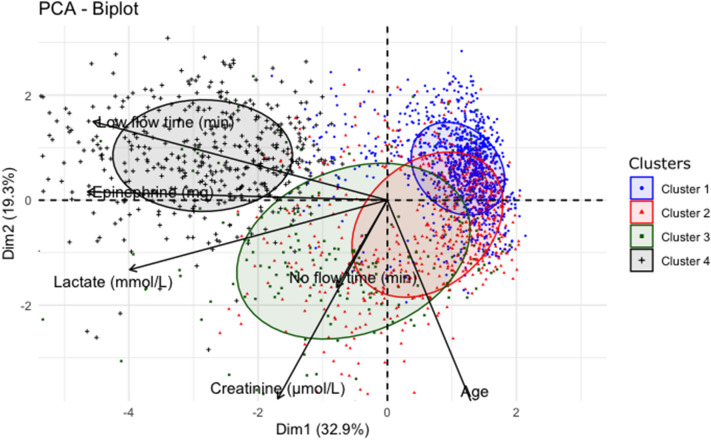
Methods: We retrospectively identified adults admitted alive to ICUs after OHCA in 2011-2018 and recorded in a prospective registry for the Paris region (France). We identified patient clusters by performing an unsupervised hierarchical cluster analysis (without mode of death among the variables) based on Utstein clinical and laboratory variables. For each cluster, we estimated the hazard ratio (HRs) for RPRS.
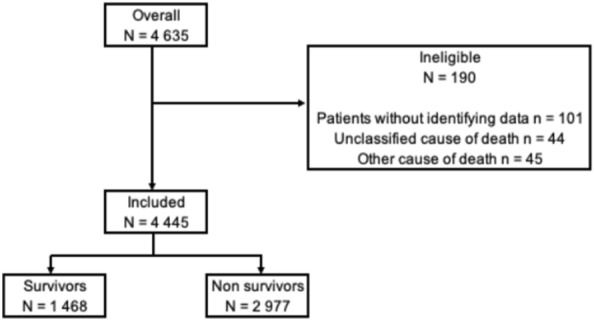
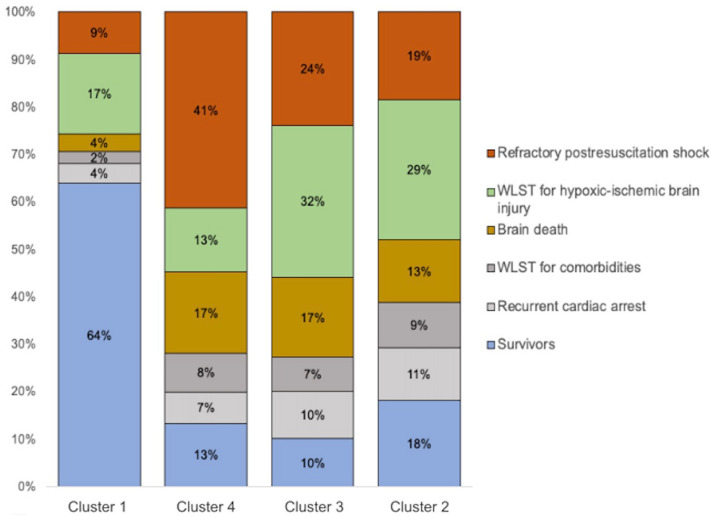
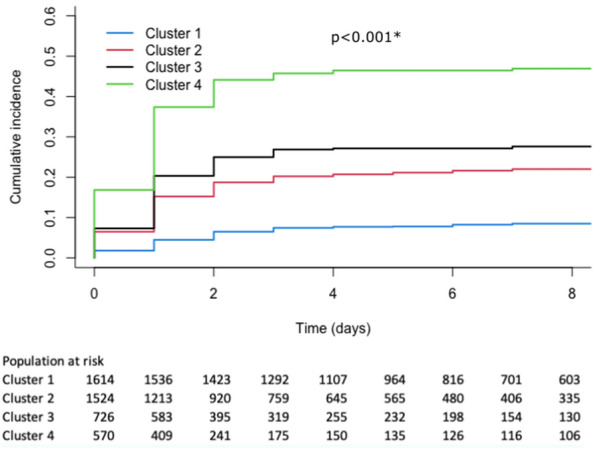
Results: Of the 4445 included patients, 1468 (33%) were discharged alive from the ICU and 2977 (67%) died in the ICU. We identified four clusters: initial shockable rhythm with short low-flow time (cluster 1), initial non-shockable rhythm with usual absence of ST-segment elevation (cluster 2), initial non-shockable rhythm with long no-flow time (cluster 3), and long low-flow time with high epinephrine dose (cluster 4). RPRS was significantly associated with this last cluster (HR, 5.51; 95% confidence interval 4.51-6.74).
Conclusions: We identified patient clusters based on Utstein criteria, and one cluster was strongly associated with RPRS. This result may help to make decisions about using specific treatments after OHCA.
Keywords: Mode of death; Personalized medicine; Post-resuscitation; Shock; Sudden death.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bougouin W, Lamhaut L, Marijon E, Jost D, Dumas F, Deye N, et al. Characteristics and prognosis of sudden cardiac death in Greater Paris: population-based approach from the Paris Sudden Death Expertise Center (Paris-SDEC) Intensive Care Med. 2014;40:846–854. doi: 10.1007/s00134-014-3252-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
