

Estimated Reductions in Opioid Overdose Deaths With Sustainment of Public Health Interventions in 4 US States
- PMID: 37294571
- PMCID: PMC10257094
- DOI: 10.1001/jamanetworkopen.2023.14925
Estimated Reductions in Opioid Overdose Deaths With Sustainment of Public Health Interventions in 4 US States
Abstract
Importance: In 2021, more than 80 000 US residents died from an opioid overdose. Public health intervention initiatives, such as the Helping to End Addiction Long-term (HEALing) Communities Study (HCS), are being launched with the goal of reducing opioid-related overdose deaths (OODs).
Objective: To estimate the change in the projected number of OODs under different scenarios of the duration of sustainment of interventions, compared with the status quo.
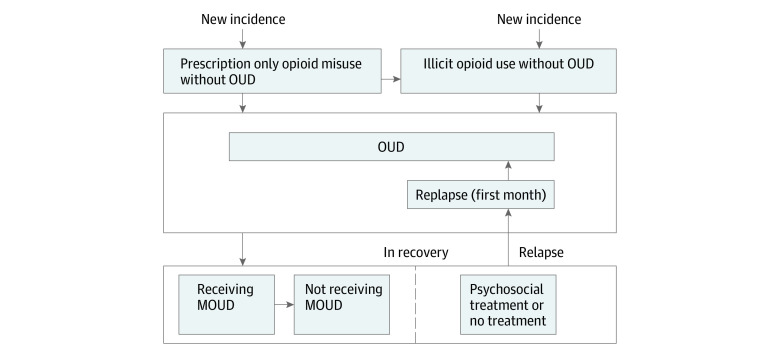
Design, setting, and participants: This decision analytical model simulated the opioid epidemic in the 4 states participating in the HCS (ie, Kentucky, Massachusetts, New York, and Ohio) from 2020 to 2026. Participants were a simulated population transitioning from opioid misuse to opioid use disorder (OUD), overdose, treatment, and relapse. The model was calibrated using 2015 to 2020 data from the National Survey on Drug Use and Health, the US Centers for Disease Control and Prevention, and other sources for each state. The model accounts for reduced initiation of medications for OUD (MOUDs) and increased OODs during the COVID-19 pandemic.
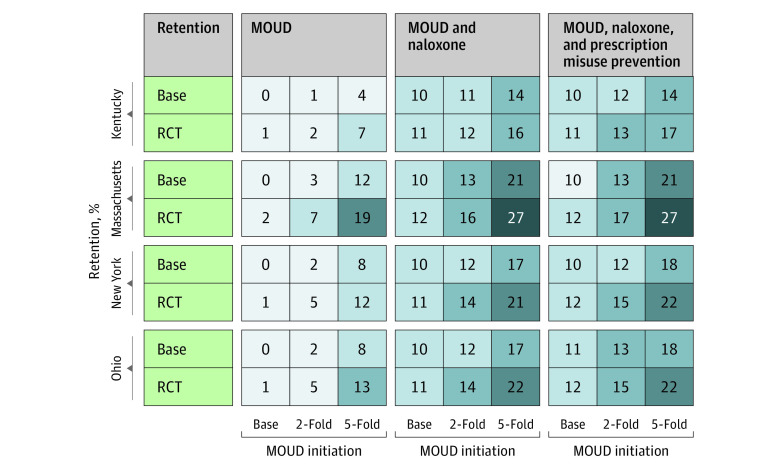
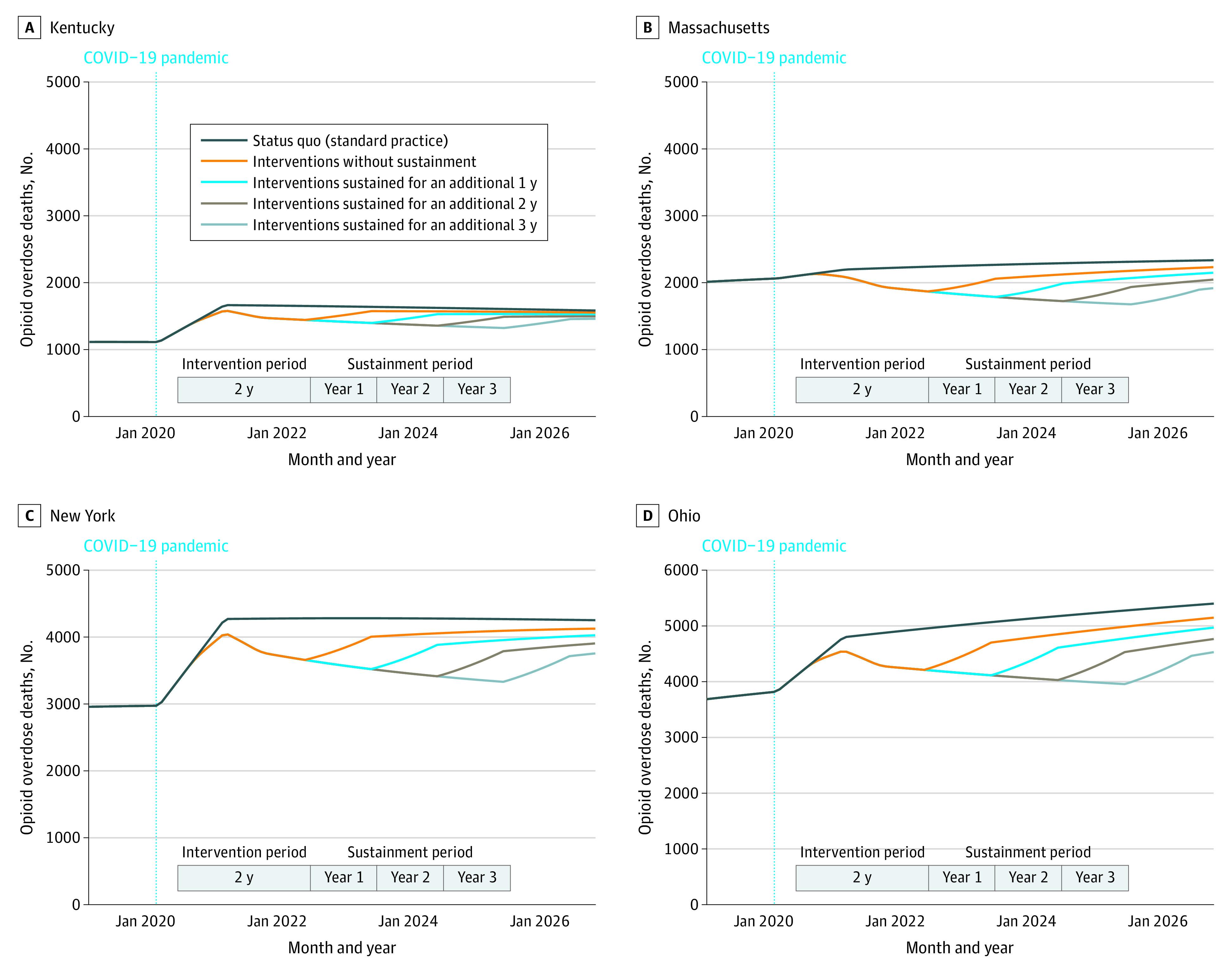
Exposure: Increasing MOUD initiation by 2- or 5-fold, improving MOUD retention to the rates achieved in clinical trial settings, increasing naloxone distribution efforts, and furthering safe opioid prescribing. An initial 2-year duration of interventions was simulated, with potential sustainment for up to 3 additional years.
Main outcomes and measures: Projected reduction in number of OODs under different combinations and durations of sustainment of interventions.
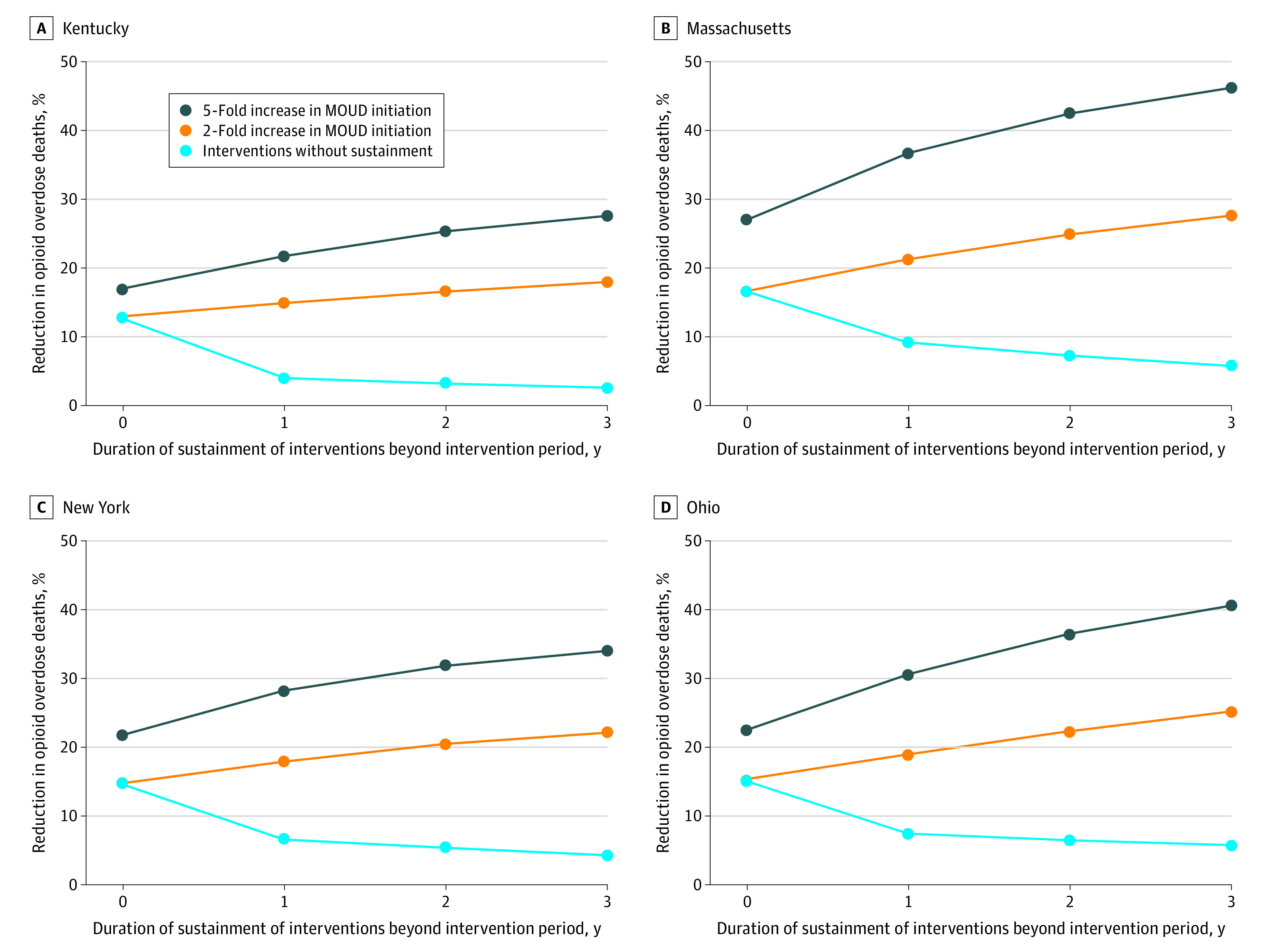
Results: Compared with the status quo, the estimated annual reduction in OODs at the end of the second year of interventions was 13% to 17% in Kentucky, 17% to 27% in Massachusetts, 15% to 22% in New York, and 15% to 22% in Ohio. Sustaining all interventions for an additional 3 years was estimated to reduce the annual number of OODs at the end of the fifth year by 18% to 27% in Kentucky, 28% to 46% in Massachusetts, 22% to 34% in New York, and 25% to 41% in Ohio. The longer the interventions were sustained, the better the outcomes; however, these positive gains would be washed out if interventions were not sustained.
Conclusions and relevance: In this decision analytical model study of the opioid epidemic in 4 US states, sustained implementation of interventions, including increased delivery of MOUDs and naloxone supply, was found to be needed to reduce OODs and prevent deaths from increasing again.
Trial registration: ClinicalTrials.gov NCT04111939.
Conflict of interest statement
Figures
Comment in
-
Paving the Way for Community-Engaged Modeling in Public Health and Other Sectors.JAMA Netw Open. 2023 Jun 1;6(6):e2317606. doi: 10.1001/jamanetworkopen.2023.17606. JAMA Netw Open. 2023. PMID: 37294574 No abstract available.
References
-
- US Department of Health and Human Services. HHS Acting Secretary declares public health emergency to address national opioid crisis. October 26, 2017. Accessed August 7, 2022. https://www.hhs.gov/about/news/2017/10/26/hhs-acting-secretary-declares-...
-
- Ahmad F, Rossen L, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. Accessed May 23, 2022. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
