

Surgical Versus Non-Surgical Treatment for Thoracolumbar Burst Fractures Without Neurological Deficit: A Systematic Review and Meta-Analysis
- PMID: 37294595
- PMCID: PMC10802528
- DOI: 10.1177/21925682231181875
Surgical Versus Non-Surgical Treatment for Thoracolumbar Burst Fractures Without Neurological Deficit: A Systematic Review and Meta-Analysis
Abstract
Study design: A systematic review and meta-analysis.
Objective: To update the systematic review comparing the outcomes between surgical and non-surgical treatment for thoracolumbar burst fractures without neurological deficit.
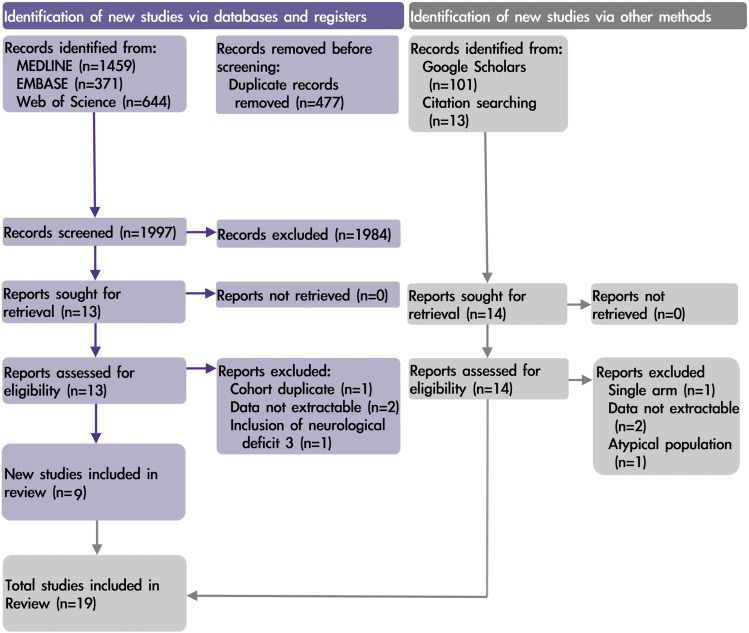
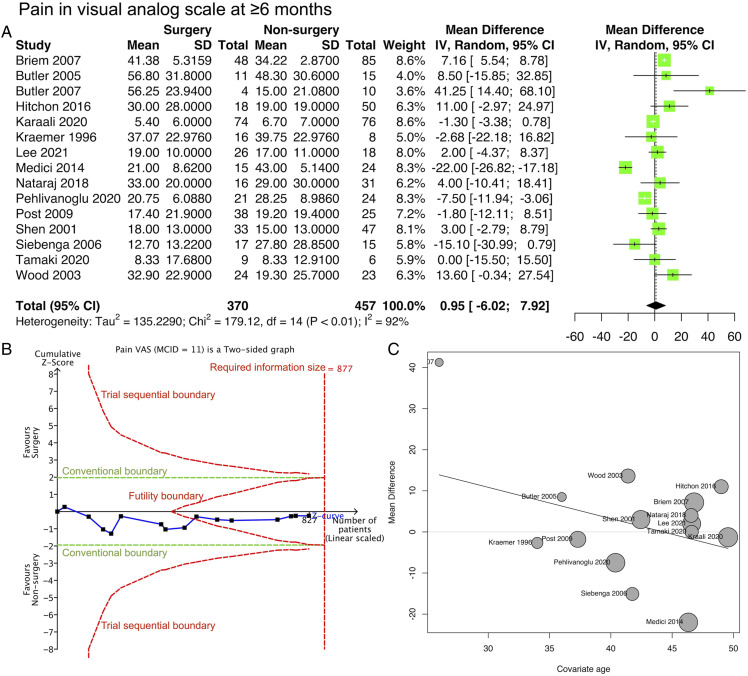
Methods: We registered a protocol in PROSPERO (ID: CRD42021291769) and searched Medline, Embase, Web of Science, and Google Scholar databases. Surgical and non-surgical treatments were compared in patients with thoracolumbar burst fractures without neurological deficits. Predefined outcomes at ≥6 months included pain (defined as a visual analog scale [VAS] of 0-100), functional outcomes (Oswestry Disability Index [ODI] of 0-50 and Roland-Morris Disability Questionnaire [RMDQ] of 0-24), and kyphotic angulation.
Results: Nineteen studies involving 1056 patients were included in the analyses. For outcomes at ≥6 months, little to no difference was found in pain VAS score (mean difference, .95 [95% confidence interval {CI}, -6.02 to 7.92]; 827 participants; 15 studies; I2 = 92%), ODI (mean difference, -1.40 [95% CI, -5.11 to 2.31]; 446 participants; 7 studies; I2 = 79%), and RMDQ (mean difference, -.73 [95% CI, -5.13 to 3.66]; 216 participants; 5 studies; I2 = 77%). The kyphotic angulation in the surgery group was 6.35° lower than that in the non-surgery group (mean difference, -6.56° [95% CI, -10.26° to -2.87°]; 527 participants; ten studies; I2 = 86%). The trial sequential analysis indicated all outcomes reached adequate statistical power. The certainty of the evidence for all 4 outcomes was very low. For the analysis of minimally invasive procedures compared to traditional open surgeries, a statistically significant subgroup difference was found for VAS and ODI (P < .01 and P < .04, respectively).
Conclusion: Surgical and non-surgical treatments showed little or no difference in outcomes at ≥6 months. This review provides a conclusion with adequate statistical power by including non-randomized studies. However, non-randomized studies also lowered the certainty of the evidence to a very low level.
Keywords: non-surgery; surgery; thoracolumbar burst fractures.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



Similar articles
-
Treatment of thoracolumbar burst fractures: extended follow-up of a randomized clinical trial comparing orthosis versus no orthosis.J Neurosurg Spine. 2017 Jul;27(1):42-47. doi: 10.3171/2016.11.SPINE161031. Epub 2017 Apr 14. J Neurosurg Spine. 2017. PMID: 28409669 Clinical Trial.
-
Unipedicular-Screw Index Vertebra Manipulation Technique for Minimally Invasive Short-Segment Thoracolumbar Fracture Fixation.Int J Spine Surg. 2023 Oct;17(5):652-660. doi: 10.14444/8524. Epub 2023 Jul 24. Int J Spine Surg. 2023. PMID: 37487671 Free PMC article.
-
Nonoperative versus operative treatment for thoracolumbar burst fractures without neurologic deficit: a meta-analysis.Clin Orthop Relat Res. 2012 Feb;470(2):567-77. doi: 10.1007/s11999-011-2157-7. Epub 2011 Nov 5. Clin Orthop Relat Res. 2012. PMID: 22057820 Free PMC article. Review.
-
Effects of Bracing on Clinical and Radiographic Outcomes Following Thoracolumbar Burst Fractures in Neurologically Intact Patients: A Meta-Analysis of Randomized Controlled Trials.JBJS Rev. 2019 Sep;7(9):e9. doi: 10.2106/JBJS.RVW.19.00006. JBJS Rev. 2019. PMID: 31567716
-
Thoracolumbar Burst Fractures: A Systematic Review and Meta-Analysis Comparing Posterior-Only Instrumentation Versus Combined Anterior-Posterior Instrumentation.Spine (Phila Pa 1976). 2021 Aug 1;46(15):E840-E849. doi: 10.1097/BRS.0000000000003934. Spine (Phila Pa 1976). 2021. PMID: 34228696
Cited by
-
Analysis of factors influencing the intravertebral shell phenomenon after posterior reduction internal fixation of thoracolumbar fracture: a retrospective study.BMC Musculoskelet Disord. 2024 Jan 10;25(1):49. doi: 10.1186/s12891-024-07168-9. BMC Musculoskelet Disord. 2024. PMID: 38200488 Free PMC article.
-
Biomechanical Effect of Different Posterior Fixation Techniques on Stability and Adjacent Segment Degeneration in Treating Thoracolumbar Burst Fracture With Osteoporosis: A Finite Element Analysis.Spine (Phila Pa 1976). 2024 Aug 1;49(15):E229-E238. doi: 10.1097/BRS.0000000000005034. Epub 2024 May 9. Spine (Phila Pa 1976). 2024. PMID: 38721831 Free PMC article.
-
The effectiveness of posterior Schanz screw system in the anatomical restoration of thoracolumbar vertebral burst fractures: A 10-year single-institution experience.J Craniovertebr Junction Spine. 2024 Oct-Dec;15(4):411-418. doi: 10.4103/jcvjs.jcvjs_118_24. Epub 2025 Jan 15. J Craniovertebr Junction Spine. 2024. PMID: 40061203 Free PMC article.
-
Percutaneous reduction of thoracolumbar fractures using monoaxial screws: Comparison of two instruments based on initial reduction and loss of reduction.Brain Spine. 2024 Mar 1;4:102778. doi: 10.1016/j.bas.2024.102778. eCollection 2024. Brain Spine. 2024. PMID: 38584864 Free PMC article.
References
-
- Bradford DS, McBride GG. Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits. Clin Orthop. 1987;218:201-216. - PubMed
-
- Yi L, Bai J, Jin G, Wu T, Baoleri X, The Cochrane Collaboration . Operative versus non-operative treatment for thoracolumbar burst fractures without neurological deficit. In: Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley and Sons, Ltd; 2006. doi:10.1002/14651858.CD005079.pub2 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
