

Eltrombopag for Low-Risk Myelodysplastic Syndromes With Thrombocytopenia: Interim Results of a Phase II, Randomized, Placebo-Controlled Clinical Trial (EQOL-MDS)
- PMID: 37294914
- PMCID: PMC10552995
- DOI: 10.1200/JCO.22.02699
Eltrombopag for Low-Risk Myelodysplastic Syndromes With Thrombocytopenia: Interim Results of a Phase II, Randomized, Placebo-Controlled Clinical Trial (EQOL-MDS)
Abstract
Purpose: In myelodysplastic syndromes (MDS), severe thrombocytopenia is associated with poor prognosis. This multicenter trial presents the second-part long-term efficacy and safety results of eltrombopag in patients with low-risk MDS and severe thrombocytopenia.
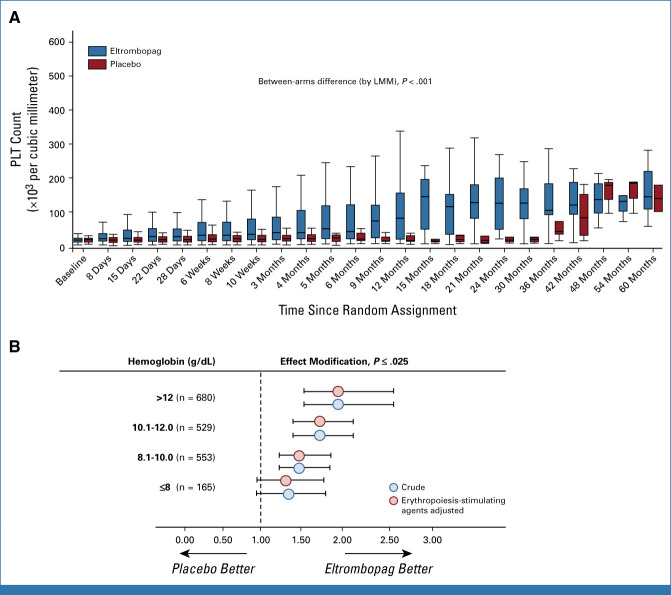
Methods: In this single-blind, randomized, placebo-controlled, phase-II trial of adult patients with International Prognostic Scoring System low- or intermediate-1-risk MDS, patients with a stable platelet (PLT) count (<30 × 103/mm3) received eltrombopag or placebo until disease progression. Primary end points were duration of PLT response (PLT-R; calculated from the time of PLT-R to date of loss of PLT-R, defined as bleeding/PLT count <30 × 103/mm3 or last date in observation) and long-term safety and tolerability. Secondary end points included incidence and severity of bleeding, PLT transfusions, quality of life, leukemia-free survival, progression-free survival, overall survival and pharmacokinetics.
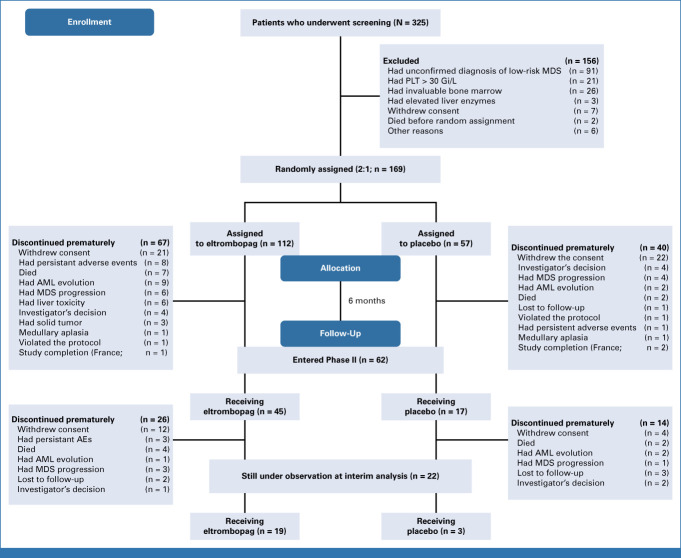
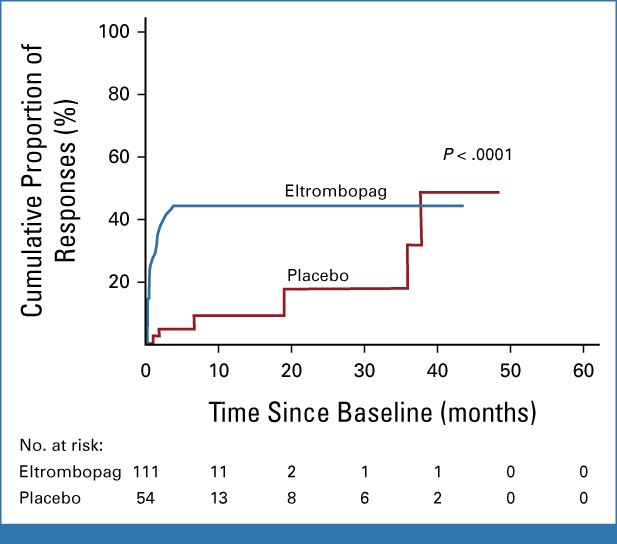
Results: From 2011 to 2021, of 325 patients screened, 169 patients were randomly assigned oral eltrombopag (N = 112) or placebo (N = 57) at a starting dose of 50 mg once daily to maximum of 300 mg. PLT-R, with 25-week follow-up (IQR, 14-68) occurred in 47/111 (42.3%) eltrombopag patients versus 6/54 (11.1%) in placebo (odds ratio, 5.9; 95% CI, 2.3 to 14.9; P < .001). In eltrombopag patients, 12/47 (25.5%) lost the PLT-R, with cumulative thrombocytopenia relapse-free survival at 60 months of 63.6% (95% CI, 46.0 to 81.2). Clinically significant bleeding (WHO bleeding score ≥ 2) occurred less frequently in the eltrombopag arm than in the placebo group (incidence rate ratio, 0.54; 95% CI, 0.38 to 0.75; P = .0002). Although no difference in the frequency of grade 1-2 adverse events (AEs) was observed, a higher proportion of eltrombopag patients experienced grade 3-4 AEs (χ2 = 9.5, P = .002). AML evolution and/or disease progression occurred in 17% (for both) of eltrombopag and placebo patients with no difference in survival times.
Conclusion: Eltrombopag was effective and relatively safe in low-risk MDS with severe thrombocytopenia. This trial is registered with ClinicalTrials.gov identifier: NCT02912208 and EU Clinical Trials Register: EudraCT No. 2010-022890-33.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
Comment in
-
Eltrombopag in Lower-Risk Myelodysplastic Syndrome: Revival of Its Use in Thrombocytopenia.J Clin Oncol. 2023 Oct 1;41(28):4465-4468. doi: 10.1200/JCO.23.01141. Epub 2023 Jul 10. J Clin Oncol. 2023. PMID: 37428990 No abstract available.
References
-
- Brunning R, Orazi A, Germing U: Myelodysplastic syndromes/neoplasms, overview, in Swerdlow SH, Campo E, Harris NL, et al. (eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (ed 4). Lyon, France, IARC Press, 2008
-
- Garcia-Manero G, Shan J, Faderl S, et al. : A prognostic score for patients with lower risk myelodysplastic syndrome. Leukemia 22:538-543, 2008 - PubMed
-
- Waisbren J, Dinner S, Altman J, et al. : Disease characteristics and prognosis of myelodysplastic syndrome presenting with isolated thrombocytopenia. Int J Hematol 105:44-51, 2017 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
