

Kinesin-5 inhibition improves neural regeneration in experimental autoimmune neuritis
- PMID: 37296476
- PMCID: PMC10257330
- DOI: 10.1186/s12974-023-02822-w
Kinesin-5 inhibition improves neural regeneration in experimental autoimmune neuritis
Abstract
Background: Autoimmune neuropathies can result in long-term disability and incomplete recovery, despite adequate first-line therapy. Kinesin-5 inhibition was shown to accelerate neurite outgrowth in different preclinical studies. Here, we evaluated the potential neuro-regenerative effects of the small molecule kinesin-5 inhibitor monastrol in a rodent model of acute autoimmune neuropathies, experimental autoimmune neuritis.
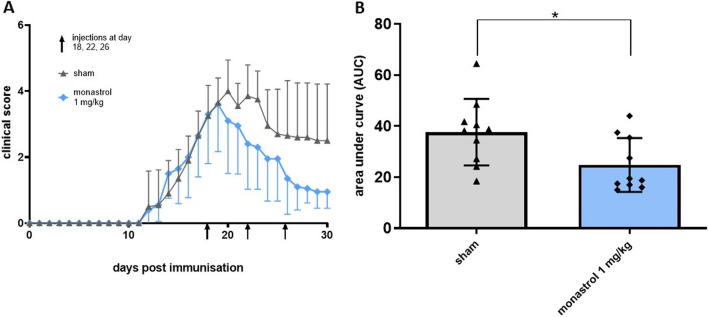
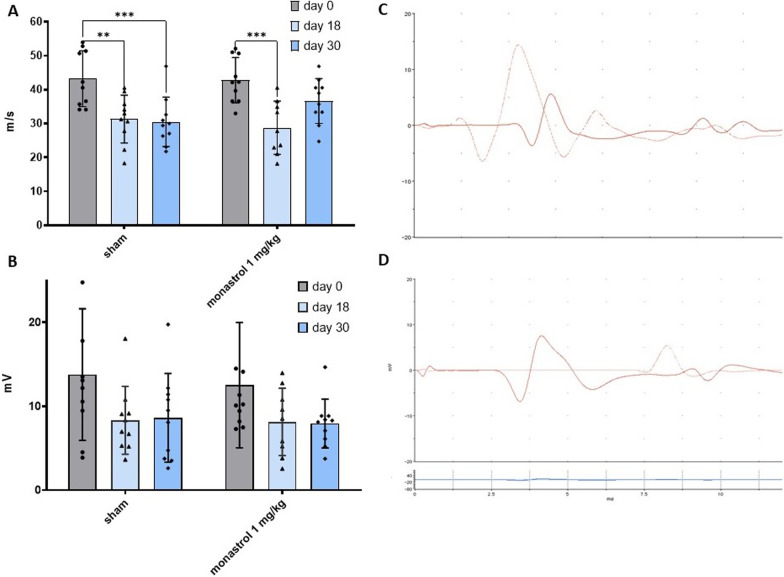
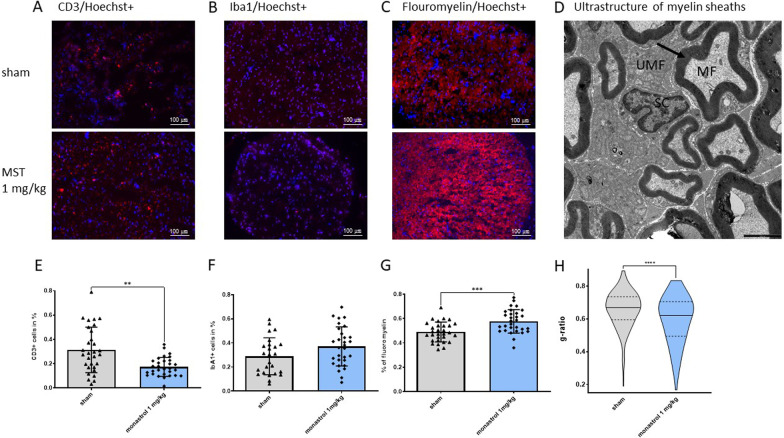
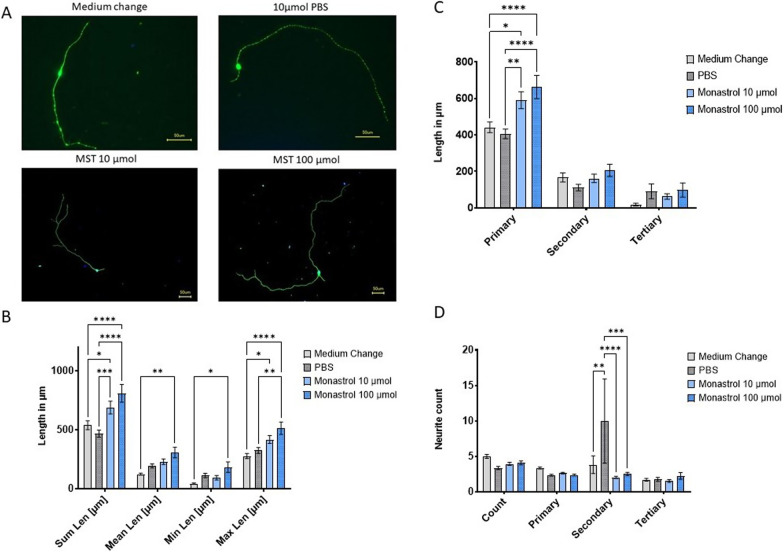
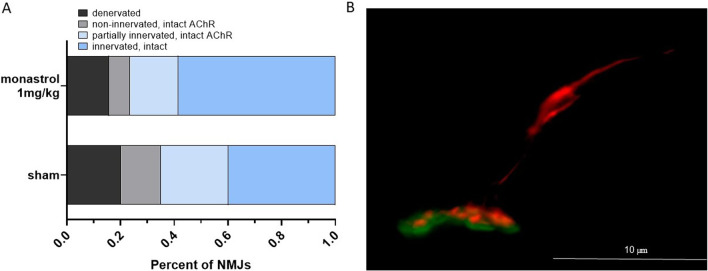
Methods: Experimental autoimmune neuritis was induced in Lewis rats with the neurogenic P2-peptide. At the beginning of the recovery phase at day 18, the animals were treated with 1 mg/kg monastrol or sham and observed until day 30 post-immunisation. Electrophysiological and histological analysis for markers of inflammation and remyelination of the sciatic nerve were performed. Neuromuscular junctions of the tibialis anterior muscles were analysed for reinnervation. We further treated human induced pluripotent stem cells-derived secondary motor neurons with monastrol in different concentrations and performed a neurite outgrowth assay.
Results: Treatment with monastrol enhanced functional and histological recovery in experimental autoimmune neuritis. Motor nerve conduction velocity at day 30 in the treated animals was comparable to pre-neuritis values. Monastrol-treated animals showed partially reinnervated or intact neuromuscular junctions. A significant and dose-dependent accelerated neurite outgrowth was observed after kinesin-5 inhibition as a possible mode of action.
Conclusion: Pharmacological kinesin-5 inhibition improves the functional outcome in experimental autoimmune neuritis through accelerated motor neurite outgrowth and histological recovery. This approach could be of interest to improve the outcome of autoimmune neuropathy patients.
Keywords: Autoimmune neuropathy; Eg5; Experimental autoimmune neuritis; Guillain–Barré syndrome; Monastrol; Neuroregeneration.
© 2023. The Author(s).
Conflict of interest statement
GRF received royalties from Springer, Thieme and Hogrefe. He declared speaker honoraria from Bayer, Desitin, Ergo DKV, Forum für medizinische Fortbildung (FomF) GmbH, GSK, Medica Academy Messe Düsseldorf, Medicbrain Healthcare, Novartis, Pfizer, and Sportärztebund NRW. HCL received honoraria for speaking and advisory board engagement or academic research support by Akcea, Alnylam, Biogen, Celgene, CSL Behring, Grifols, Gruenenthal, LFB Pharma, Takeda and UCB. The other authors declare no conflict of interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
