

Fluid-Attenuated Inversion Recovery Sequence with Fat Suppression for Assessment of Ankle Synovitis without Contrast Enhancement: Comparison with Contrast-Enhanced MRI
- PMID: 37296812
- PMCID: PMC10252366
- DOI: 10.3390/diagnostics13111960
Fluid-Attenuated Inversion Recovery Sequence with Fat Suppression for Assessment of Ankle Synovitis without Contrast Enhancement: Comparison with Contrast-Enhanced MRI
Abstract
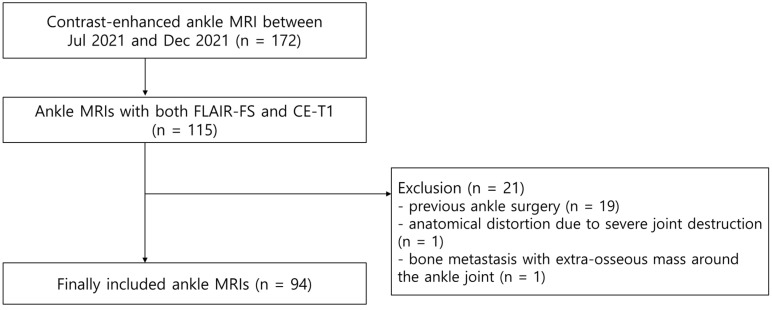
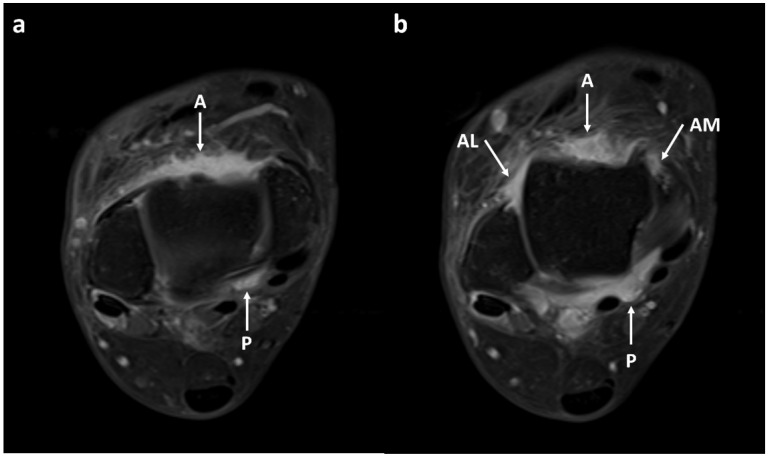
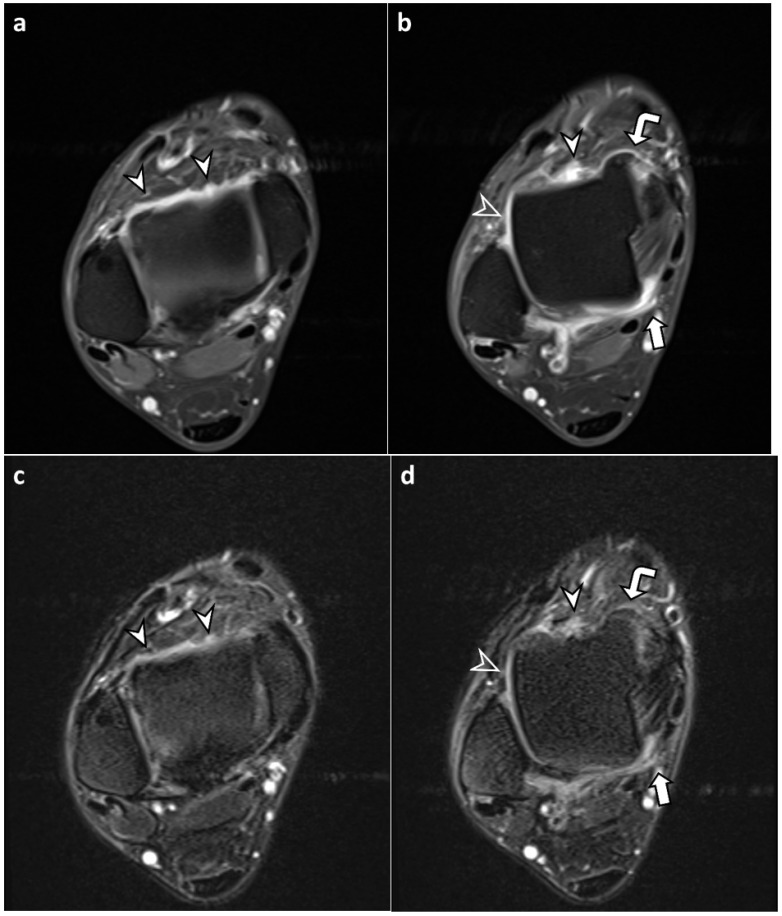
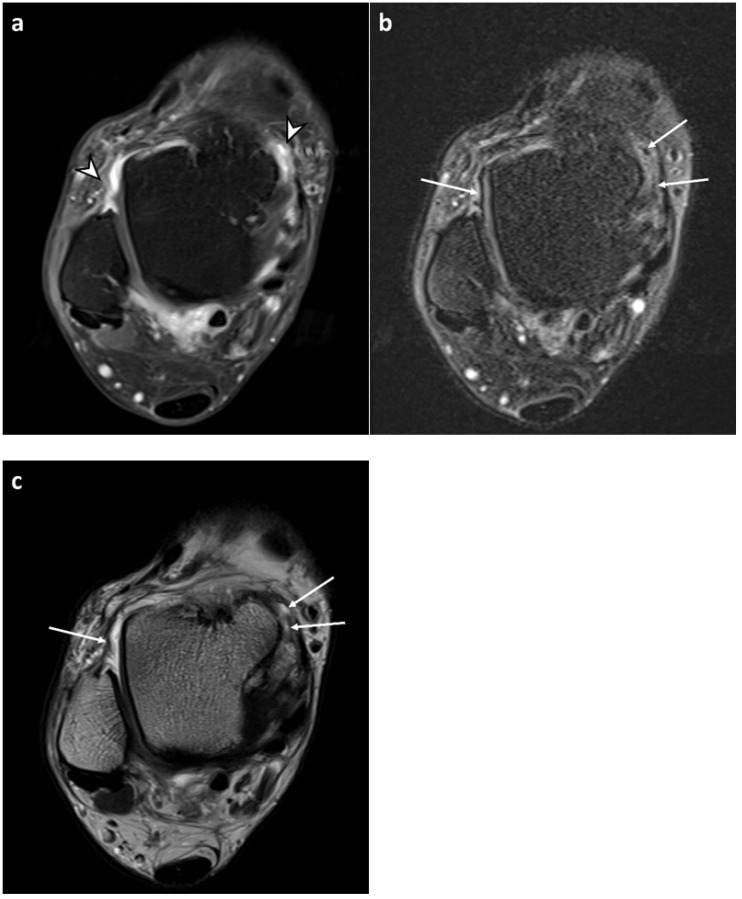
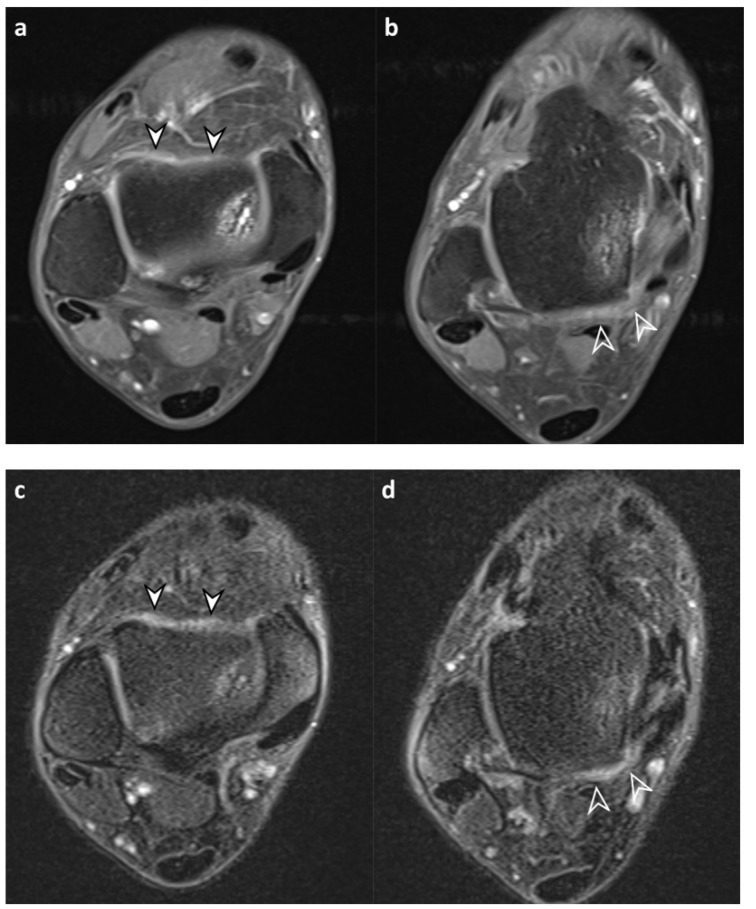
The purpose of this study was to investigate the feasibility of the fluid-attenuated inversion recovery sequence with fat suppression (FLAIR-FS) for the assessment of ankle synovitis without contrast enhancement. FLAIR-FS and contrast-enhanced, T1-weighted sequences (CE-T1) of 94 ankles were retrospectively reviewed by two radiologists. Grading of synovial visibility (four-point scale) and semi-quantitative scoring of synovial thickness (three-point scale) were performed in four compartments of the ankle in both sequences. Synovial visibility and thickness in FLAIR-FS and CE-T1 images were compared, and agreement between both sequences was assessed. Synovial visibility grades and synovial thickness scores for FLAIR-FS images were lower than those for CE-T1 images (reader 1, p = 0.016, p < 0.001; reader 2, p = 0.009, p < 0.001). Dichotomized synovial visibility grades (partial vs. full visibility) were not significantly different between both sequences. The agreement in synovial thickness scores between the FLAIR-FS and CE-T1 images was moderate to substantial (κ = 0.41-0.65). The interobserver agreement between the two readers was fair for synovial visibility (κ = 0.27-0.32) and moderate to substantial for synovial thickness (κ = 0.54-0.74). In conclusion, FLAIR-FS is a feasible MRI sequence for the evaluation of ankle synovitis without contrast enhancement.
Keywords: ankle synovitis; fluid-attenuated inversion recovery sequence; magnetic resonance imaging; synovitis imaging.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Diagnostic Accuracy of a Fluid-attenuated Inversion-Recovery Sequence with Fat Suppression for Assessment of Peripatellar Synovitis: Preliminary Results and Comparison with Contrast-enhanced MR Imaging.Radiology. 2017 Jun;283(3):769-778. doi: 10.1148/radiol.2016160155. Epub 2016 Oct 24. Radiology. 2017. PMID: 27775897
-
Comprehensive assessment of knee joint synovitis at 7 T MRI using contrast-enhanced and non-enhanced sequences.BMC Musculoskelet Disord. 2020 Feb 21;21(1):116. doi: 10.1186/s12891-020-3122-y. BMC Musculoskelet Disord. 2020. PMID: 32085776 Free PMC article.
-
Fluid-attenuated inversion-recovery sequence with fat suppression as an alternative to contrast-enhanced MRI in pediatric synovitis.Pediatr Radiol. 2024 Jan;54(1):96-104. doi: 10.1007/s00247-023-05804-5. Epub 2023 Nov 14. Pediatr Radiol. 2024. PMID: 37962605
-
Double-inversion recovery with synthetic magnetic resonance: a pilot study for assessing synovitis of the knee joint compared to contrast-enhanced magnetic resonance imaging.Eur Radiol. 2019 May;29(5):2573-2580. doi: 10.1007/s00330-018-5800-9. Epub 2018 Nov 28. Eur Radiol. 2019. PMID: 30488107
-
Intracranial meningeal disease: comparison of contrast-enhanced MR imaging with fluid-attenuated inversion recovery and fat-suppressed T1-weighted sequences.AJNR Am J Neuroradiol. 2005 Mar;26(3):553-9. AJNR Am J Neuroradiol. 2005. PMID: 15760865 Free PMC article.
Cited by
-
Recent evolution in imaging techniques for assessment of synovitis in osteoarthritis.Skeletal Radiol. 2025 Mar 22. doi: 10.1007/s00256-025-04908-3. Online ahead of print. Skeletal Radiol. 2025. PMID: 40121319 Review.
References
-
- Guermazi A., Hayashi D., Roemer F.W., Zhu Y., Niu J., Crema M.D., Javaid M.K., Marra M.D., Lynch J.A., El-Khoury G.Y., et al. Synovitis in knee osteoarthritis assessed by contrast-enhanced magnetic resonance imaging (MRI) is associated with radiographic tibiofemoral osteoarthritis and MRI-detected widespread cartilage damage: The MOST study. J. Rheumatol. 2014;41:501–508. doi: 10.3899/jrheum.130541. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
