

Conventional and Advanced Magnetic Resonance Imaging Assessment of Non-Enhancing Peritumoral Area in Brain Tumor
- PMID: 37296953
- PMCID: PMC10252005
- DOI: 10.3390/cancers15112992
Conventional and Advanced Magnetic Resonance Imaging Assessment of Non-Enhancing Peritumoral Area in Brain Tumor
Abstract
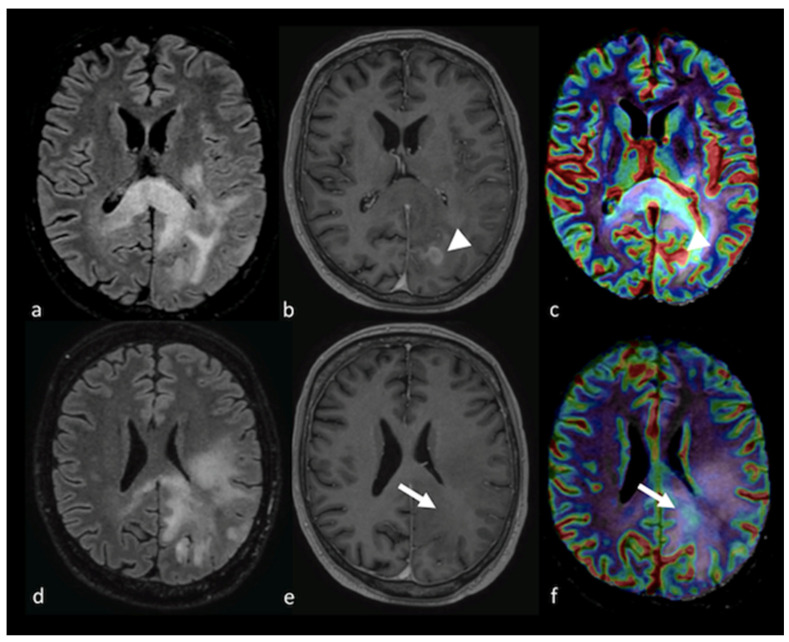
The non-enhancing peritumoral area (NEPA) is defined as the hyperintense region in T2-weighted and fluid-attenuated inversion recovery (FLAIR) images surrounding a brain tumor. The NEPA corresponds to different pathological processes, including vasogenic edema and infiltrative edema. The analysis of the NEPA with conventional and advanced magnetic resonance imaging (MRI) was proposed in the differential diagnosis of solid brain tumors, showing higher accuracy than MRI evaluation of the enhancing part of the tumor. In particular, MRI assessment of the NEPA was demonstrated to be a promising tool for distinguishing high-grade gliomas from primary lymphoma and brain metastases. Additionally, the MRI characteristics of the NEPA were found to correlate with prognosis and treatment response. The purpose of this narrative review was to describe MRI features of the NEPA obtained with conventional and advanced MRI techniques to better understand their potential in identifying the different characteristics of high-grade gliomas, primary lymphoma and brain metastases and in predicting clinical outcome and response to surgery and chemo-irradiation. Diffusion and perfusion techniques, such as diffusion tensor imaging (DTI), diffusional kurtosis imaging (DKI), dynamic susceptibility contrast-enhanced (DSC) perfusion imaging, dynamic contrast-enhanced (DCE) perfusion imaging, arterial spin labeling (ASL), spectroscopy and amide proton transfer (APT), were the advanced MRI procedures we reviewed.
Keywords: MRI; advanced techniques; brain tumors; neuroradiology; peritumoral edema.
Conflict of interest statement
The authors declare no conflict of interest.
Figures











References
-
- Lin X., Lee M., Buck O., Woo K.M., Zhang Z., Hatzoglou V., Omuro A., Arevalo-Perez J., Thomas A.A., Huse J., et al. Diagnostic Accuracy of T1-Weighted Dynamic Contrast-Enhanced-MRI and DWI-ADC for Differentiation of Glioblastoma and Primary CNS Lymphoma. AJNR Am. J. Neuroradiol. 2017;38:485–491. doi: 10.3174/ajnr.A5023. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
