

Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study
- PMID: 37297212
- PMCID: PMC10254387
- DOI: 10.3390/ma16114080
Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study
Abstract
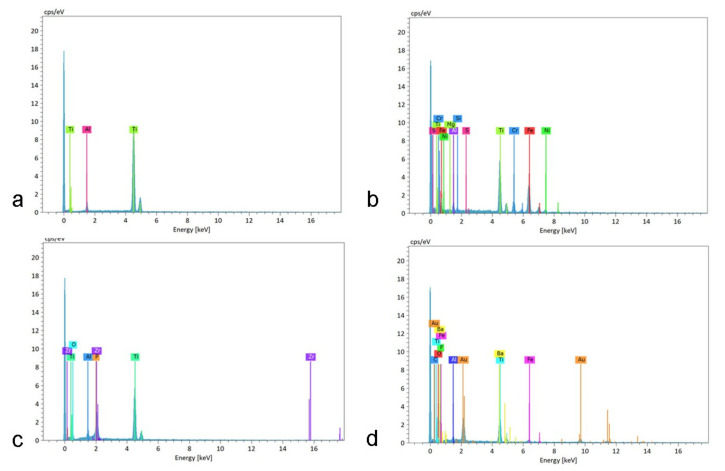
The long-term success of dental implant rehabilitation depends significantly on proper peri-implant soft tissue integration. Therefore, decontamination of abutments prior to their connection to the implant is beneficial to enhance soft tissue attachment and to aid in maintaining marginal bone around the implant. Consequently, different implant abutment decontamination protocols were evaluated regarding biocompatibility, surface morphology, and bacterial load. The protocols evaluated were autoclave sterilization, ultrasonic washing, steam cleaning, chlorhexidine chemical decontamination, and sodium hypochlorite chemical decontamination. The control groups included: (1) implant abutments prepared and polished in a dental lab without decontamination and (2) unprepared implant abutments obtained directly from the company. Surface analysis was performed using scanning electron microscopy (SEM). Biocompatibility was evaluated using XTT cell viability and proliferation assays. Biofilm biomass and viable counts (CFU/mL) (n = 5 for each test) were used for surface bacterial load evaluation. Surface analysis revealed areas of debris and accumulation of materials, such as iron, cobalt, chromium, and other metals, in all abutments prepared by the lab and with all decontamination protocols. Steam cleaning was the most efficient method for reducing contamination. Chlorhexidine and sodium hypochlorite left residual materials on the abutments. XTT results showed that the chlorhexidine group (M = 0.7005, SD = 0.2995) had the lowest values (p < 0.001) (autoclave: M = 3.6354, SD = 0.1510; ultrasonic: M = 3.4077, SD = 0.3730; steam: M = 3.2903, SD = 0.2172; NaOCl: M = 3.5377, SD = 0.0927; prep non-decont.: M = 3.4815, SD = 0.2326; factory: M = 3.6173, SD = 0.0392). Bacterial growth (CFU/mL) was high in the abutments treated with steam cleaning and ultrasonic bath: 2.93 × 109, SD = 1.68 × 1012 and 1.83 × 109, SD = 3.95 × 1010, respectively. Abutments treated with chlorhexidine showed higher toxicity to cells, while all other samples showed similar effects to the control. In conclusion, steam cleaning seemed to be the most efficient method for reducing debris and metallic contamination. Bacterial load can be reduced using autoclaving, chlorhexidine, and NaOCl.
Keywords: decontamination; osseointegration; peri-implantitis; steam; titanium; ultrasonics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures









References
-
- Pjetursson B.E., Sailer I., Latyshev A., Rabel K., Kohal R.J., Karasan D. A systematic review and meta-analysis evaluating the survival, the failure, and the complication rates of veneered and monolithic all-ceramic implant-supported single crowns. Clin. Oral Implants Res. 2021;32((Suppl. S21)):254–288. doi: 10.1111/clr.13863. - DOI - PMC - PubMed
-
- Pjetursson B.E., Thoma D., Jung R., Zwahlen M., Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implants Res. 2012;23((Suppl. S6)):22–38. doi: 10.1111/j.1600-0501.2012.02546.x. - DOI - PubMed
-
- Jung R.E., Zembic A., Pjetursson B.E., Zwahlen M., Thoma D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implants Res. 2012;23((Suppl. S6)):2–21. doi: 10.1111/j.1600-0501.2012.02547.x. - DOI - PubMed
-
- Welander M., Abrahamsson I., Berglundh T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implants Res. 2008;19:635–641. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
