

Unravelling the Clinical Co-Morbidity and Risk Factors Associated with Agenesis of the Corpus Callosum
- PMID: 37297816
- PMCID: PMC10253475
- DOI: 10.3390/jcm12113623
Unravelling the Clinical Co-Morbidity and Risk Factors Associated with Agenesis of the Corpus Callosum
Abstract
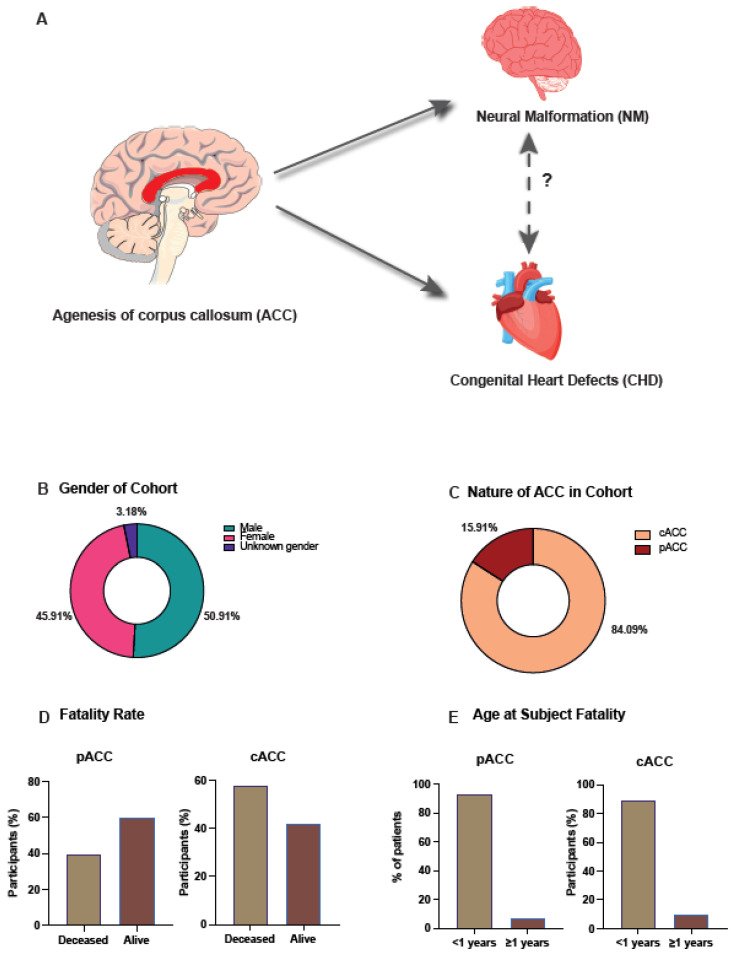
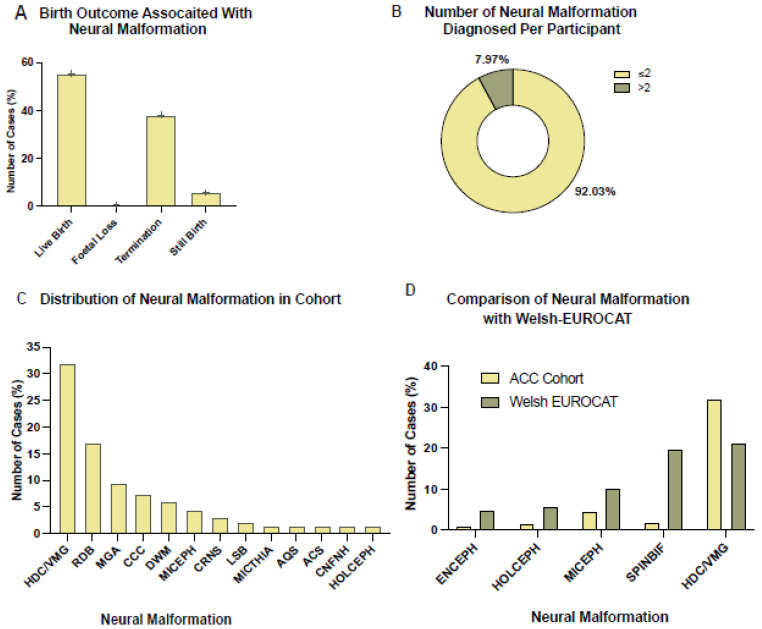
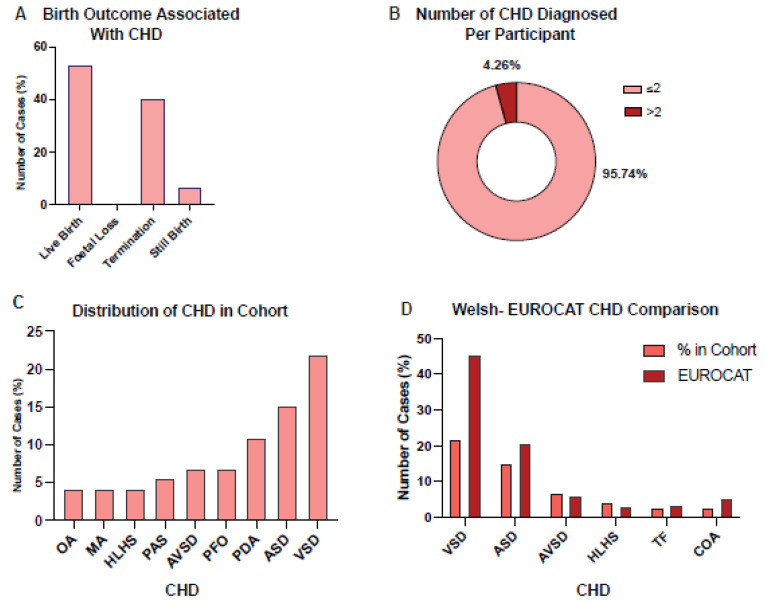
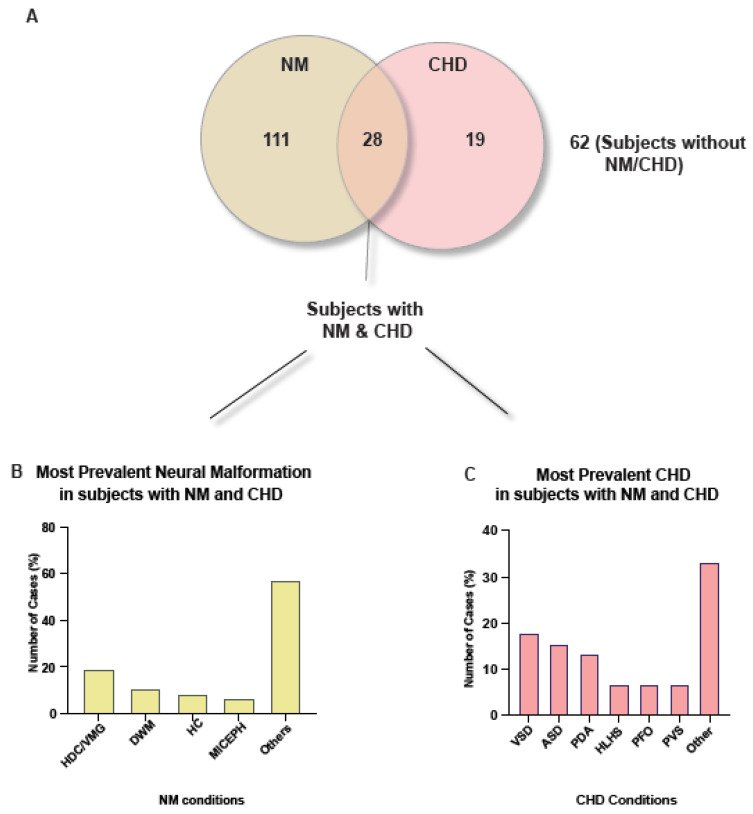
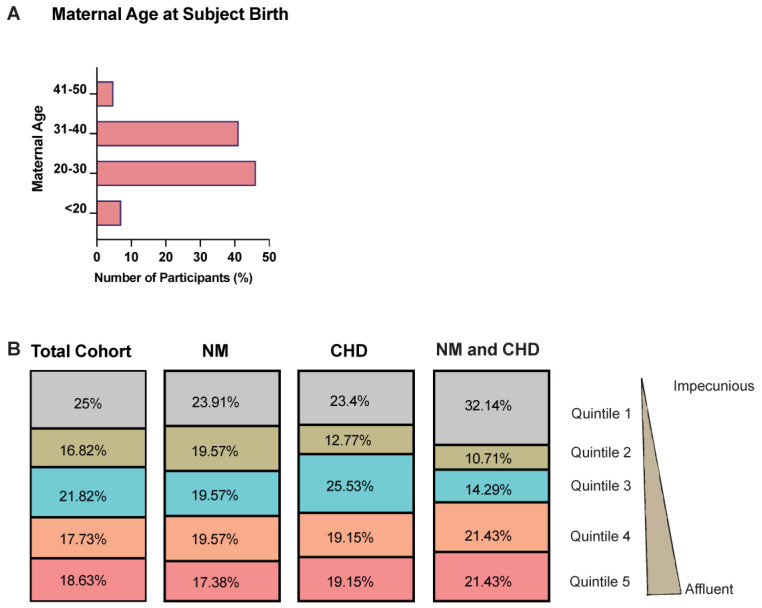
Agenesis of the Corpus Callosum (ACC) can result in multiple neurological deficits including social and behavioural issues. However, the underlying aetiology, clinical co-morbidity and the contributing risk factors remain elusive, resulting in inaccurate prognosis and delayed therapy. The main objective of this study was to comprehensively describe the epidemiology and clinical co-morbidity associated with patients diagnosed with ACC. The secondary objective was to identify the factors that contribute towards increased risk for ACC. For this, we analysed 22 years (1998-2020) of clinical data across the whole of Wales, UK collected through the Congenital Anomaly Register & Information Service (CARIS) and Public Health Wales (PHW). Our results demonstrate that complete ACC (84.1%) was the prevalent subtype, in comparison to partial ACC. Further, ventriculomegaly/hydrocephalus (26.37%) and ventricular septal defect (21.92%) were identified to be the most prevalent neural malformation (NM) and congenital heart disorder (CHD) in our cohort. Although 12.7% of subjects with ACC had both an NM and CHD, we found no significant association between them (χ2 (1, n = 220) = 3.84, p = 0.33). We found socioeconomic deprivation and increased maternal age contributed towards an increased risk for ACC. To the best of our knowledge, this study for the first time defines the clinical phenotypes and the factors that contribute to ACC within the Welsh population. These findings will be of value to both patients and healthcare professionals, who may take preventative or remedial measures.
Keywords: agenesis of corpus callosum; comorbidity; congenital heart disorders; neurodevelopmental disorders; risk factors.
Conflict of interest statement
All other authors declared no conflict of interest.
Figures
Similar articles
-
Isolated complete agenesis of corpus callosum.Acta Paediatr Taiwan. 2003 Jan-Feb;44(1):5-7. Acta Paediatr Taiwan. 2003. PMID: 12800376
-
Outcome of Agenesis of the Corpus Callosum Diagnosed by Fetal MRI.Pediatr Neurol. 2022 Oct;135:44-51. doi: 10.1016/j.pediatrneurol.2022.07.007. Epub 2022 Jul 19. Pediatr Neurol. 2022. PMID: 35988419
-
An analysis of 109 fetuses with prenatal diagnosis of complete agenesis of corpus callosum.Neurol Sci. 2020 Jun;41(6):1521-1529. doi: 10.1007/s10072-019-04224-4. Epub 2020 Jan 22. Neurol Sci. 2020. PMID: 31970575
-
Agenesis of the corpus callosum: a clinical approach to diagnosis.Am J Med Genet C Semin Med Genet. 2014 Jun;166C(2):184-97. doi: 10.1002/ajmg.c.31405. Epub 2014 May 27. Am J Med Genet C Semin Med Genet. 2014. PMID: 24866859 Review.
-
Genetic heterogeneity in corpus callosum agenesis.Front Genet. 2022 Sep 30;13:958570. doi: 10.3389/fgene.2022.958570. eCollection 2022. Front Genet. 2022. PMID: 36246626 Free PMC article. Review.
References
-
- Schell-Apacik C.C., Wagner K., Bihler M., Ertl-Wagner B., Heinrich U., Klopocki E., Kalscheuer V.M., Muenke M., von Voss H. Agenesis and dysgenesis of the corpus callosum: Clinical, genetic and neuroimaging findings in a series of 41 patients. Am. J. Med. Genet. A. 2008;146A:2501–2511. doi: 10.1002/ajmg.a.32476. - DOI - PMC - PubMed
-
- Kamnasaran D. Corpus Callosum: Agenesis. In: Squire L., editor. Encyclopedia of Neuroscience. Elsevier; Amsterdam, The Netherlands: 2009. pp. 163–173.
LinkOut - more resources
Full Text Sources
