

Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment
- PMID: 37297888
- PMCID: PMC10253496
- DOI: 10.3390/jcm12113693
Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment
Abstract
Background: the successful treatment of spondylodiscitis (SD) and isolated spinal epidural empyema (ISEE) depends on early detection of causative pathogens, which is commonly performed either via blood cultures, intraoperative specimens, and/or image-guided biopsies. We evaluated the diagnostic sensitivity of these three procedures and assessed how it is influenced by antibiotics.
Methods: we retrospectively analyzed data from patients with SD and ISEE treated surgically at a neurosurgery university center in Germany between 2002 and 2021.
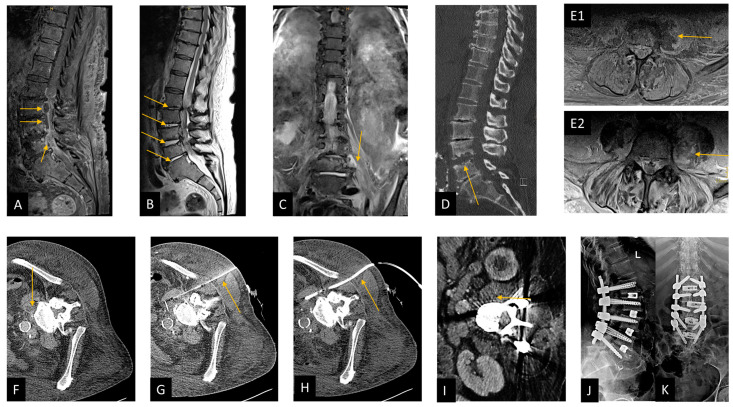
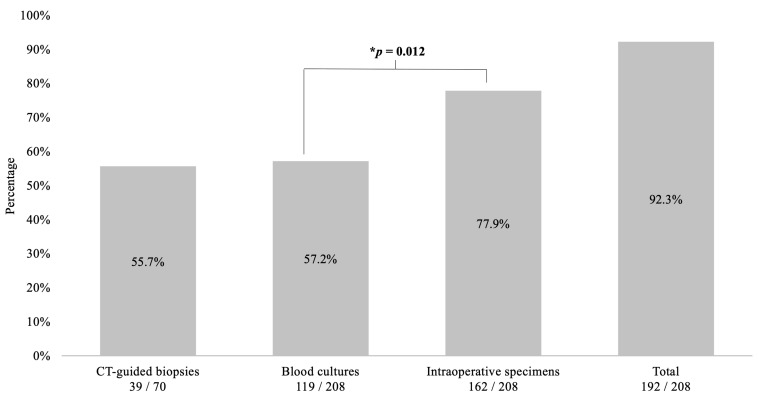
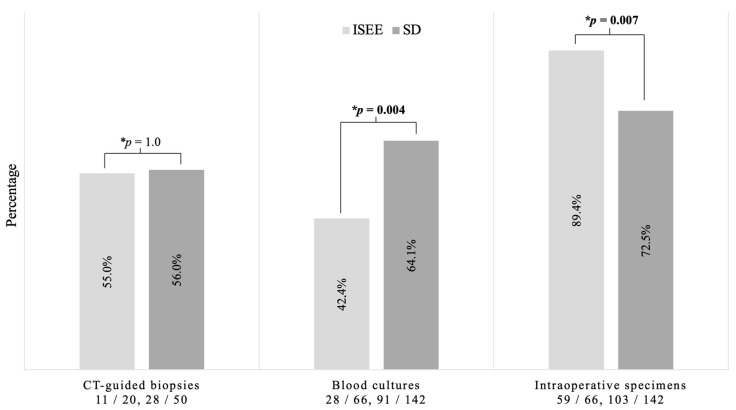
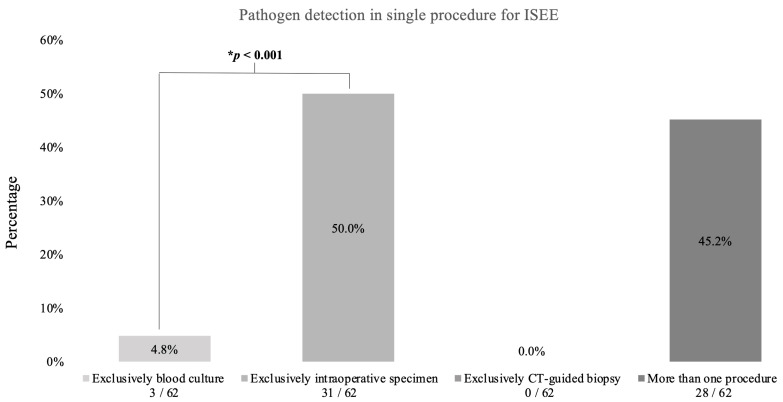
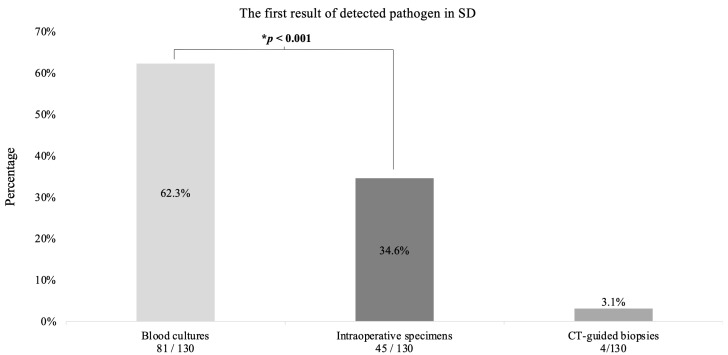
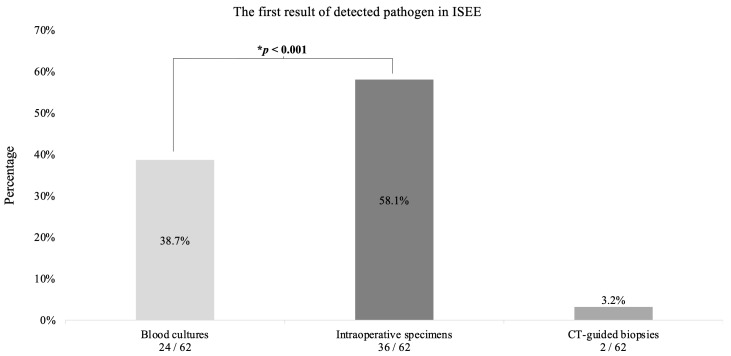
Results: we included 208 patients (68 [23-90] years, 34.6% females, 68% SD). Pathogens were identified in 192 cases (92.3%), including 187 (97.4%) pyogenic and five (2.6%) non-pyogenic infections, with Gram-positive bacteria accounting for 86.6% (162 cases) and Gram-negative for 13.4% (25 cases) of the pyogenic infections. The diagnostic sensitivity was highest for intraoperative specimens at 77.9% (162/208, p = 0.012) and lowest for blood cultures at 57.2% (119/208) and computed tomography (CT)-guided biopsies at 55.7% (39/70). Blood cultures displayed the highest sensitivity in SD patients (SD: 91/142, 64.1% vs. ISEE: 28/66, 42.4%, p = 0.004), while intraoperative specimens were the most sensitive procedure in ISEE (SD: 102/142, 71.8% vs. ISEE: 59/66, 89.4%, p = 0.007). The diagnostic sensitivity was lower in SD patients with ongoing empiric antibiotic therapy (EAT) than in patients treated postoperatively with targeted antibiotic therapy (TAT) (EAT: 77/89, 86.5% vs. TAT: 53/53, 100%, p = 0.004), whereas no effect was observed in patients with ISEE (EAT: 47/51, 92.2% vs. TAT: 15/15, 100%, p = 0.567).
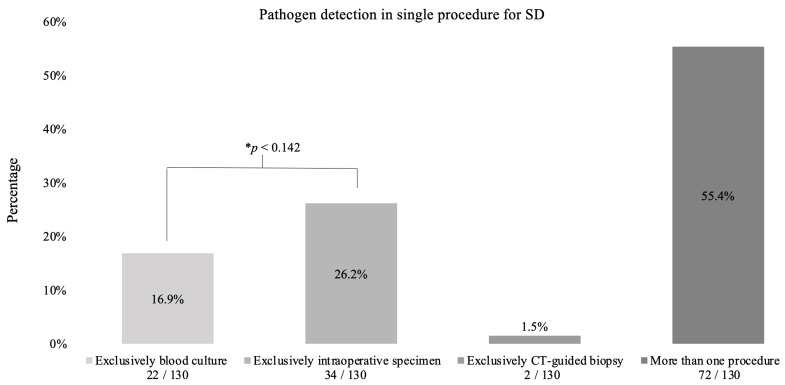
Conclusions: in our cohort, intraoperative specimens displayed the highest diagnostic sensitivity especially for ISEE, whereas blood cultures appear to be the most sensitive for SD. The sensitivity of these tests seems modifiable by preoperative EAT in patients with SD, but not in those with ISEE, underscoring the distinct differences between both pathologies.
Keywords: blood culture; computed tomography-guided biopsy; diagnostic sensitivity; intraoperative specimen; isolated spinal epidural empyema; spondylodiscitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tsiodras S., Falagas M.E. Clinical assessment and medical treatment of spine infections. Clin. Orthop. Relat. Res. 2006;444:38–50. doi: 10.1097/01.blo.0000203454.82264.cd. - DOI - PubMed
LinkOut - more resources
Full Text Sources
