

Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs
- PMID: 37297919
- PMCID: PMC10253351
- DOI: 10.3390/jcm12113724
Multimodal Prehabilitation in Heart Transplant Recipients Improves Short-Term Post-Transplant Outcomes without Increasing Costs
Abstract
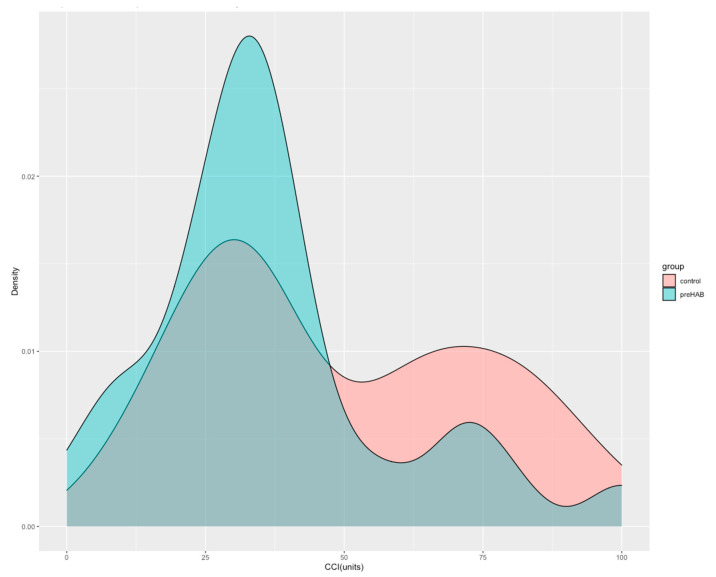
(1) Background and aim: This study aimed to investigate the impact of prehabilitation on the postoperative outcomes of heart transplantation and its cost-effectiveness. (2) Methods: This single-center, ambispective cohort study included forty-six candidates for elective heart transplantation from 2017 to 2021 attending a multimodal prehabilitation program consisting of supervised exercise training, physical activity promotion, nutritional optimization, and psychological support. The postoperative course was compared to a control cohort consisting of patients transplanted from 2014 to 2017 and those contemporaneously not involved in prehabilitation. (3) Results: A significant improvement was observed in preoperative functional capacity (endurance time 281 vs. 728 s, p < 0.001) and quality-of-life (Minnesota score 58 vs. 47, p = 0.046) after the program. No exercise-related events were registered. The prehabilitation cohort showed a lower rate and severity of postoperative complications (comprehensive complication index 37 vs. 31, p = 0.033), lower mechanical ventilation time (37 vs. 20 h, p = 0.032), ICU stay (7 vs. 5 days, p = 0.01), total hospitalization stay (23 vs. 18 days, p = 0.008) and less need for transfer to nursing/rehabilitation facilities after hospital discharge (31% vs. 3%, p = 0.009). A cost-consequence analysis showed that prehabilitation did not increase the total surgical process costs. (4) Conclusions: Multimodal prehabilitation before heart transplantation has benefits on short-term postoperative outcomes potentially attributable to enhancement of physical status, without cost-increasing.
Keywords: aerobic capacity; cost-analysis; heart transplantation; postoperative complications; prehabilitation; preoperative optimization.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures



References
-
- Crespo-Leiro M.G., Metra M., Lund L.H., Milicic D., Costanzo M.R., Filippatos G., Gustafsson F., Tsui S., Barge-Caballero E., De Jonge N., et al. Advanced heart failure: A position statement of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018;20:1505–1535. doi: 10.1002/ejhf.1236. - DOI - PubMed
-
- Yancy C.W., Jessup M., Bozkurt B., Butler J., Casey D.E., Jr., Colvin M.M., Drazner M.H., Filippatos G.S., Fonarow G.C., Givertz M.M., et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of Ame. J. Am. Coll. Cardiol. 2017;70:776–803. doi: 10.1016/j.jacc.2017.04.025. - DOI - PubMed
-
- Bottiger B.A., Nicoara A., Snyder L.D., Wischmeyer P.E., Schroder J.N., Patel C.B., Daneshmand M.A., Sladen R.N., Ghadimi K. Frailty in the End-Stage Lung Disease or Heart Failure Patient: Implications for the Perioperative Transplant Clinician. J. Cardiothorac. Vasc. Anesth. 2019;33:1382–1392. doi: 10.1053/j.jvca.2018.08.002. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
