

Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women
- PMID: 37298047
- PMCID: PMC10253627
- DOI: 10.3390/jcm12113852
Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women
Abstract
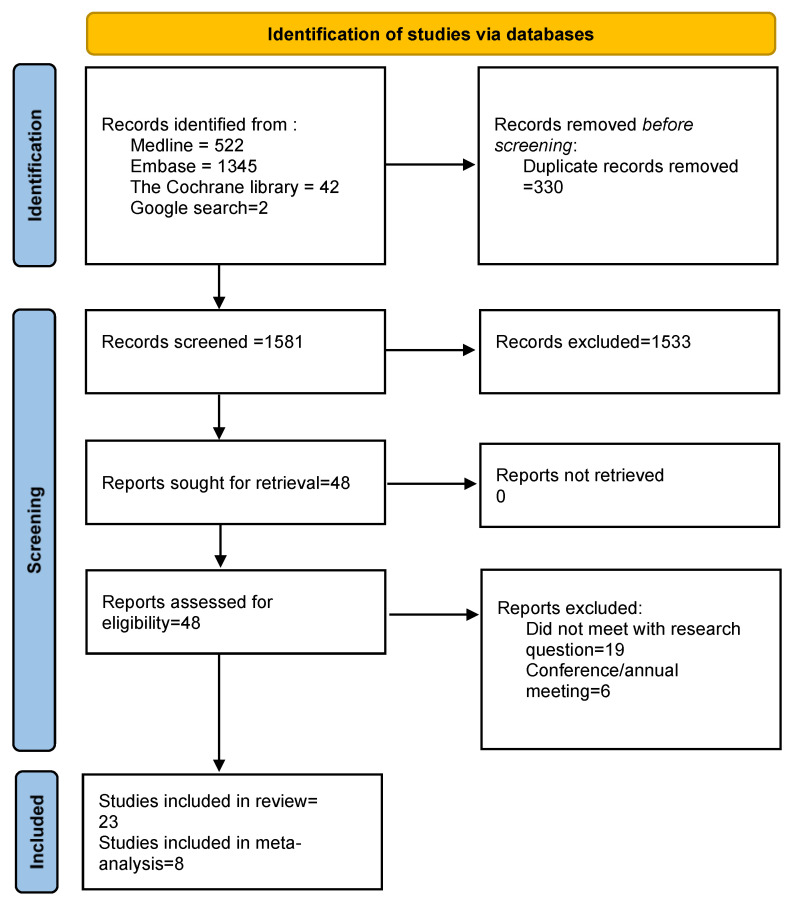
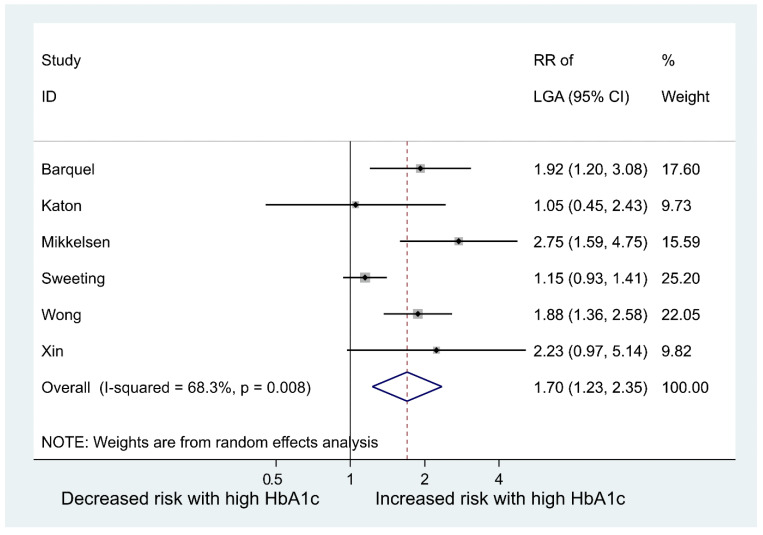
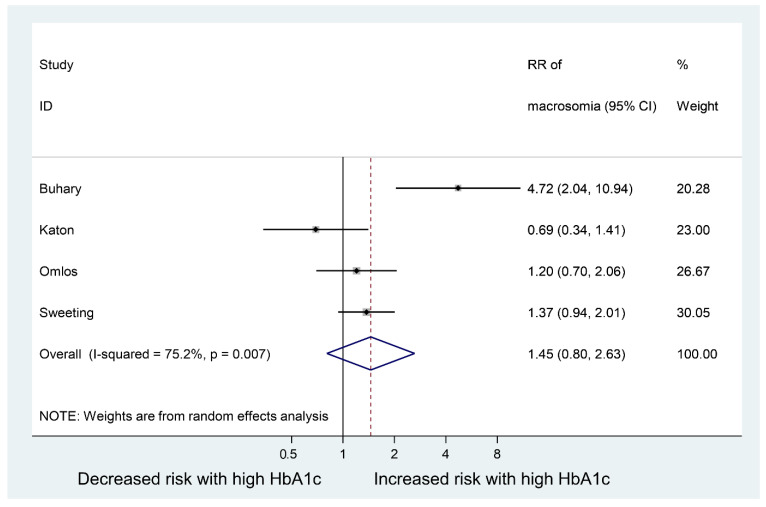
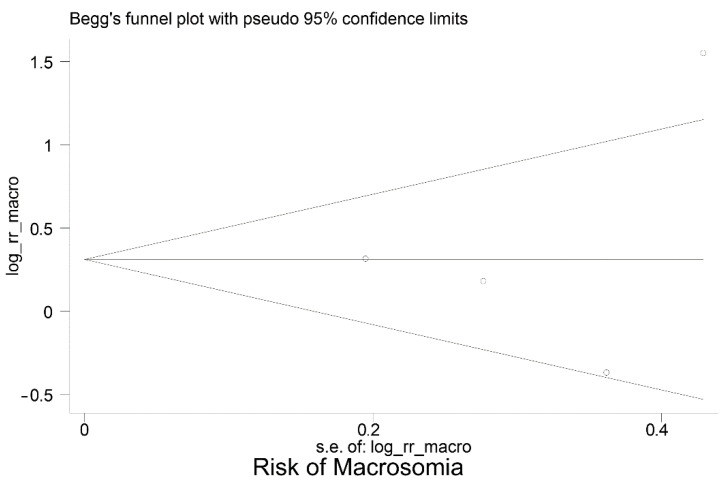
Gestational diabetes mellitus (GDM) is the most common metabolic disorder in pregnancy. GDM is associated with serious maternal and fetal complications, in particular, fetal macrosomia and large for gestational age (LGA), which predisposes to a higher risk of childhood obesity and type 2 diabetes mellitus later in life. Early prediction and diagnosis of GDM leads to early interventions such as diet and lifestyle, which could mitigate the maternal and fetal complications associated with GDM. Glycated haemoglobin A1c (HbA1c) has been widely used for monitoring, screening for and diagnosing diabetes and prediabetes. Increasing evidence has also showed that HbA1c could indicate fetal glucose supply. Thus, we hypothesise that the HbA1c level at around 24 to 28 weeks may predict the development of fetal macrosomia or an LGA baby in women with GDM, which could be useful for better prevention of fetal macrosomia and LGA. We searched MEDLINE, EMBASE, Cochrane and Google Scholar databases from inception to November 2022 for relevant studies that reported at least one HbA1c level during 24-28 weeks of pregnancy and fetal macrosomia or an LGA baby. We excluded studies that were not published in the English language. No other search filters were applied during the search. Two independent reviewers selected eligible studies for meta-analysis. Two independent reviewers performed data collection and analyses. The PROSPERO registration number is CRD42018086175. A total of 23 studies were included in this systematic review. Of these, 8 papers reported data of 17,711 women with GDM that allowed for inclusion in a meta-analysis. The obtained results demonstrated the prevalence of fetal macrosomia was 7.4% and of LGA, 13.36%. Meta-analyses showed that the estimated pooled risk ratio (RR) for LGA in women with high HbA1c values compared to normal or low values was 1.70 (95% CI: 1.23-2.35), p = 0.001; and the pooled RR for fetal macrosomia was 1.45 (95% CI: 0.80 to 2.63), p = 0.215. Further research is needed to evaluate the utility of HbA1c levels in predicting the delivery of a baby with fetal macrosomia or LGA in pregnant women.
Keywords: GDM; HbA1c; LGA; fetal macrosomia; gestational diabetes mellitus; glycated haemoglobin; large for gestational age.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
