

(Smoldering) multiple myeloma: mismatch between tumor load estimated from bone marrow biopsy at iliac crest and tumor load shown by MRI
- PMID: 37300710
- PMCID: PMC10582145
- DOI: 10.1007/s00256-023-04383-8
(Smoldering) multiple myeloma: mismatch between tumor load estimated from bone marrow biopsy at iliac crest and tumor load shown by MRI
Abstract
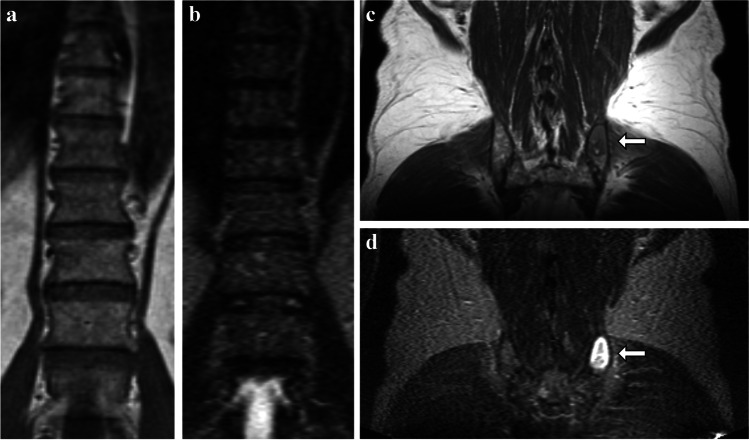
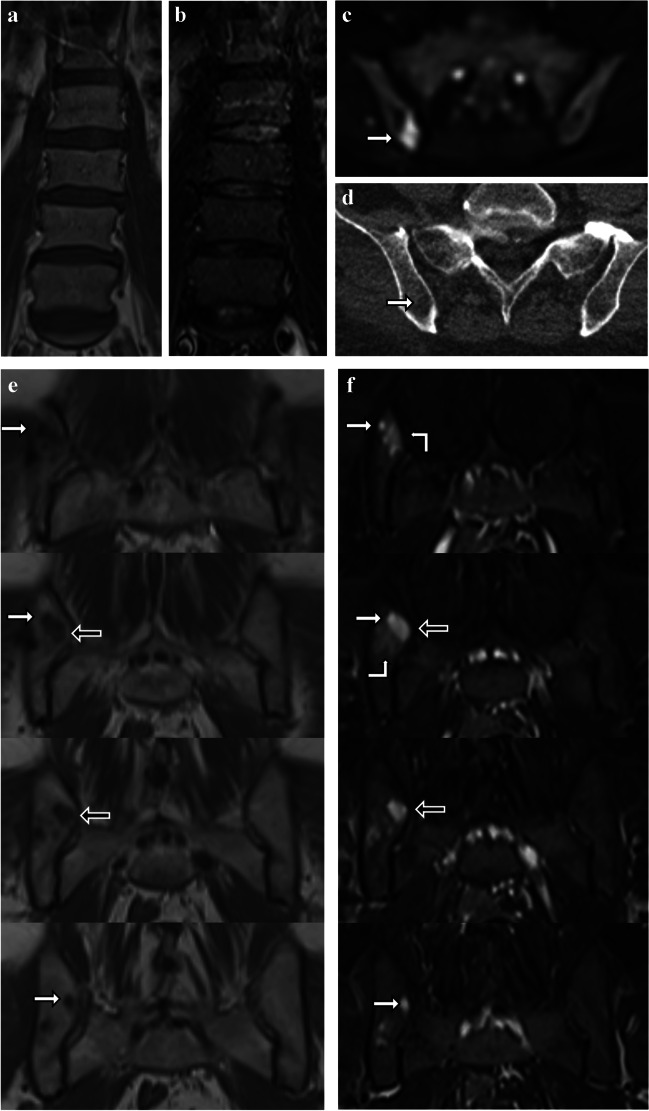
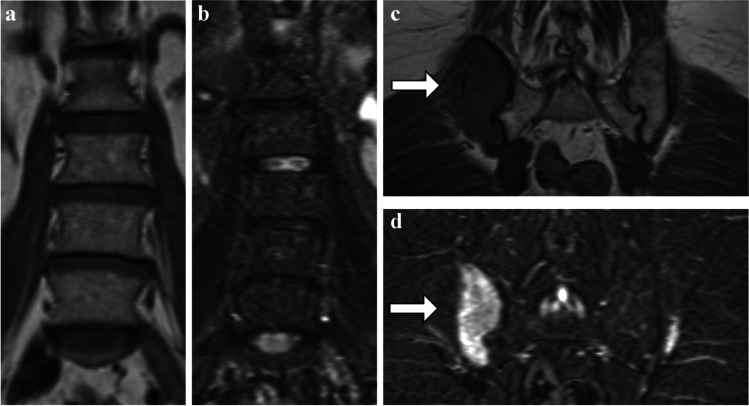
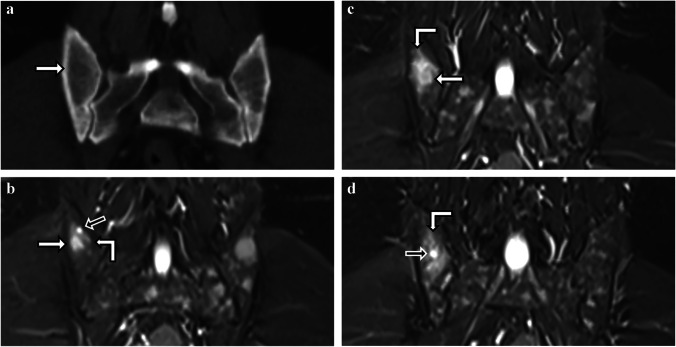
In multiple myeloma and its precursor stages, precise quantification of tumor load is of high importance for diagnosis, risk assessment, and therapy response evaluation. Both whole-body MRI, which allows to investigate the complete bone marrow of a patient, and bone marrow biopsy, which is commonly used to assess the histologic and genetic status, are relevant methods for tumor load assessment in multiple myeloma. We report on a series of striking mismatches between the plasma cell infiltration estimating the tumor load from unguided biopsies of the bone marrow at the posterior iliac crest and the tumor load assessment from whole-body MRI.
Keywords: Bone marrow biopsy; Magnetic resonance imaging; Monoclonal plasma cell disorders; Multiple myeloma; Tumor load.
© 2023. The Author(s).
Conflict of interest statement
Sandra Sauer: travel grants or honoraria for presentations for Celgene, BMS, Janssen, Takeda and Amgen. All other authors declare that they have no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
