

Extrafollicular IgD-CD27-CXCR5-CD11c- DN3 B cells infiltrate inflamed tissues in autoimmune fibrosis and in severe COVID-19
- PMID: 37300833
- PMCID: PMC10227203
- DOI: 10.1016/j.celrep.2023.112630
Extrafollicular IgD-CD27-CXCR5-CD11c- DN3 B cells infiltrate inflamed tissues in autoimmune fibrosis and in severe COVID-19
Abstract
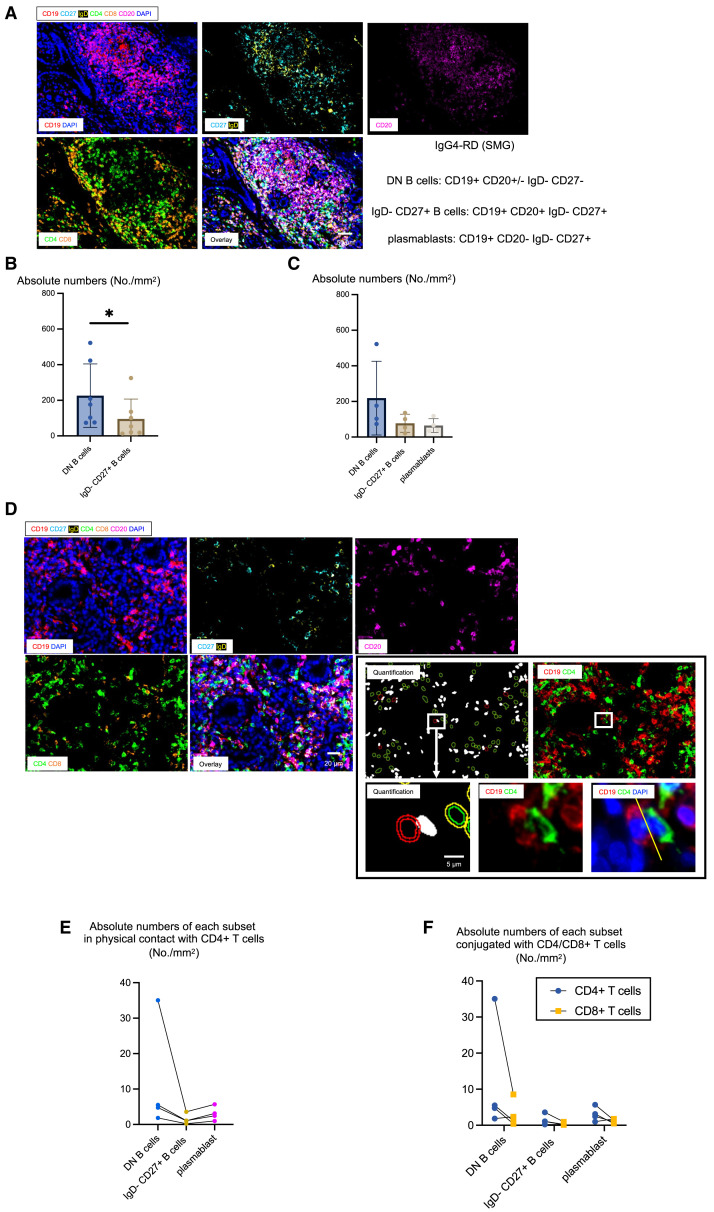
Although therapeutic B cell depletion dramatically resolves inflammation in many diseases in which antibodies appear not to play a central role, distinct extrafollicular pathogenic B cell subsets that accumulate in disease lesions have hitherto not been identified. The circulating immunoglobulin D (IgD)-CD27-CXCR5-CD11c+ DN2 B cell subset has been previously studied in some autoimmune diseases. A distinct IgD-CD27-CXCR5-CD11c- DN3 B cell subset accumulates in the blood both in IgG4-related disease, an autoimmune disease in which inflammation and fibrosis can be reversed by B cell depletion, and in severe COVID-19. These DN3 B cells prominently accumulate in the end organs of IgG4-related disease and in lung lesions in COVID-19, and double-negative B cells prominently cluster with CD4+ T cells in these lesions. Extrafollicular DN3 B cells may participate in tissue inflammation and fibrosis in autoimmune fibrotic diseases, as well as in COVID-19.
Keywords: B cell depletion in disease; COVID-19 pathogenesis; CP: Immunology; DN3 B cells; IgG4-related disease; T-B collaboration in disease; double-negative B cells; extrafollicular B cells; inflammatory fibrosis.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests S.P. is on the scientific advisory boards of Abpro, Inc., BeBiopharma, Inc., Paratus Biosciences, and Octagon Therapeutics.
Figures






References
-
- Woodruff M.C., Ramonell R.P., Nguyen D.C., Cashman K.S., Saini A.S., Haddad N.S., Ley A.M., Kyu S., Howell J.C., Ozturk T., et al. Extrafollicular B cell responses correlate with neutralizing antibodies and morbidity in COVID-19. Nat. Immunol. 2020;21:1506–1516. doi: 10.1038/s41590-020-00814-z. - DOI - PMC - PubMed
-
- Kaneko N., Kuo H.H., Boucau J., Farmer J.R., Allard-Chamard H., Mahajan V.S., Piechocka-Trocha A., Lefteri K., Osborn M., Bals J., et al. Loss of Bcl-6-expressing T follicular helper cells and germinal centers in COVID-19. Cell. 2020;183:143–157.e13. doi: 10.1016/j.cell.2020.08.025. - DOI - PMC - PubMed
-
- Mattoo H., Mahajan V.S., Della-Torre E., Sekigami Y., Carruthers M., Wallace Z.S., Deshpande V., Stone J.H., Pillai S. De novo oligoclonal expansions of circulating plasmablasts in active and relapsing IgG4-related disease. J. Allergy Clin. Immunol. 2014;134:679–687. doi: 10.1016/j.jaci.2014.03.034. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
