

A systematic review and meta-analysis of randomised controlled trials on surgical treatments for ingrown toenails part I: recurrence and relief of symptoms
- PMID: 37301845
- PMCID: PMC10257290
- DOI: 10.1186/s13047-023-00631-1
A systematic review and meta-analysis of randomised controlled trials on surgical treatments for ingrown toenails part I: recurrence and relief of symptoms
Abstract
Background: Ingrown toenails are a common nail pathology. When conservative treatments are ineffective, a surgical approach is often utilised. Despite recent narrative reviews, there is a need for an up-to-date and rigorous systematic review of surgical methods for treating ingrown toenails.
Methods: Five databases (MEDLINE, Embase, CINAHL, Web of Science and CENTRAL) and two registers (Clinicaltrials.gov and ISRCTN) were searched to January 2022 for randomised trials evaluating the effects of a surgical intervention(s) for ingrown toenails with a follow-up of at least 1 month. Two independent reviewers screened records, extracted data, assessed risk of bias and certainty of evidence.
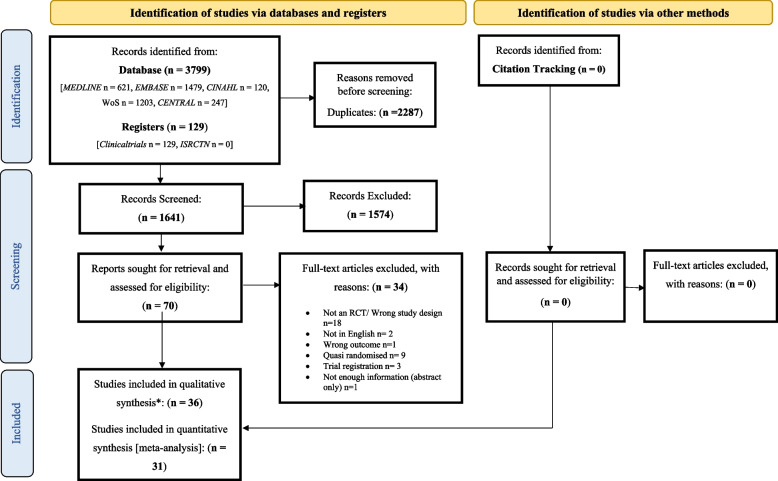
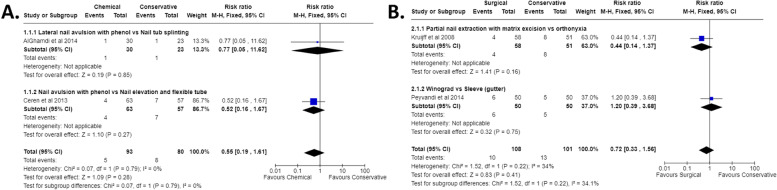
Results: Of 3,928 records identified, 36 (3,756 participants; 62.7% males) surgical interventions were included in the systematic review and 31 studies in the meta-analysis. There was very low quality evidence that using phenol with nail avulsion vs nail avulsion without phenol reduces the risk of recurrence (risk ratio [RR] 0.13 [95% CI 0.06 to 0.27], p < 0.001). No favourable effect was observed between chemical or surgical vs conservative management (0.55 [0.19 to 1.61], p = 0.280; 0.72 [0.33 to 1.56], p = 0.410), chemical or surgical vs other (e.g., CO2 laser, electrocautery) (1.61 [0.88 to 2.95], p = 0.120; 0.58 [0.25 to 1.37], p = 0.220), chemical vs surgical (0.75 [0.46 to 1.21], p = 0.230), surgical vs surgical (0.42 [0.21 to 0.85]), chemical vs chemical (0.19 [0.01 to 3.80], p = 0.280), surgical vs surgical + chemical (3.68 [0.20 to 67.35], p = 0.380), chemical vs surgical + chemical (1.92 [0.06 to 62.30], p = 0.710), local anaesthetic vs local anaesthetic + adrenaline (1.03 [0.22 to 4.86], p = 0.970), chemical timings 30 s vs 60 s (2.00 [0.19 to 21.41]) or antibiotics vs no antibiotics (0.54 [0.12 to 2.52], p = 0.430). Central toenail resection was the only procedure to significantly relieve symptoms (p = 0.001) but data were only available up to 8 weeks post-surgery.
Conclusion: Despite the high number of publications, the quality of research was poor and the conclusions that can be inferred from existing trials is limited. Phenolisation of the nail matrix appears to reduce the risk of recurrence following nail ablation, and with less certainty 1 min appears to be the optimum time for application. Despite this being a widely performed procedure there remains a lack of good quality evidence to guide practice.
Keywords: Ingrown nail; Ingrown nails; Malformed; Nail; Nail avulsion; Nail surgery; Onychocryptosis; Review; Systematic.
© 2023. The Author(s).
Conflict of interest statement
MB is a member of the Journal of Foot and Ankle Research Editorial Board.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
