

Bidirectionality between Cardiometabolic Diseases and COVID-19: Role of Humoral Immunity
- PMID: 37302794
- PMCID: PMC10256583
- DOI: 10.1016/j.advnut.2023.06.003
Bidirectionality between Cardiometabolic Diseases and COVID-19: Role of Humoral Immunity
Abstract
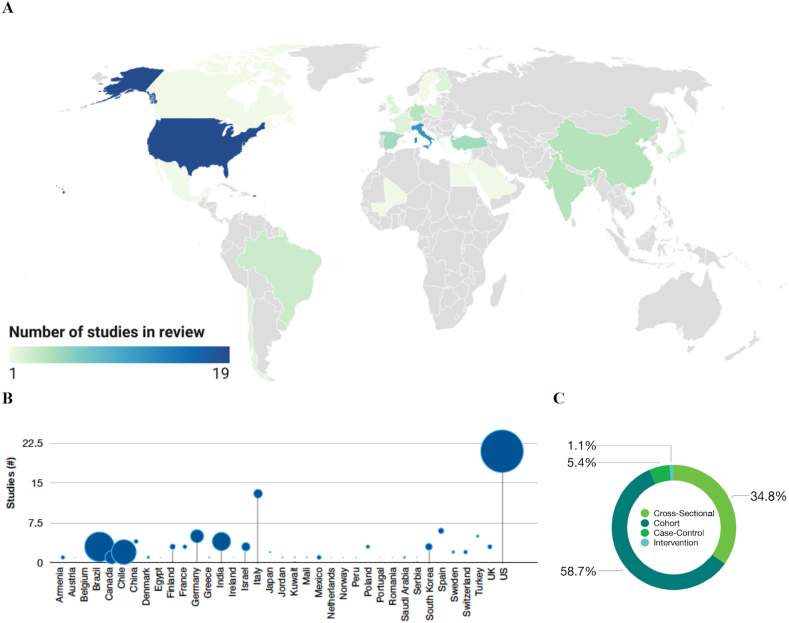
Cardiometabolic diseases and abnormalities have recently emerged as independent risk factors of coronavirus disease 2019 (COVID-19) severity, including hospitalizations, invasive mechanical ventilation, and mortality. Determining whether and how this observation translates to more effective long-term pandemic mitigation strategies remains a challenge due to key research gaps. Specific pathways by which cardiometabolic pathophysiology affects humoral immunity against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and vice versa, remain unclear. This review summarizes current evidence of the bidirectional influences between cardiometabolic diseases (diabetes, adiposity, hypertension, CVDs) and SARS-CoV-2 antibodies induced from infection and vaccination based on human studies. Ninety-two studies among >408,000 participants in 37 countries on 5 continents (Europe, Asia, Africa, and North and South America) were included in this review. Obesity was associated with higher neutralizing antibody titers following SARS-CoV-2 infection. Most studies conducted prior to vaccinations found positive or null associations between binding antibodies (levels, seropositivity) and diabetes; after vaccinations, antibody responses did not differ by diabetes. Hypertension and CVDs were not associated with SARS-CoV-2 antibodies. Findings underscore the importance of elucidating the extent that tailored recommendations for COVID-19 prevention, vaccination effectiveness, screening, and diagnoses among people with obesity could reduce disease burden caused by SARS-CoV-2.
Keywords: SARS-CoV-2; antibodies; cardiovascular diseases; diabetes; obesity.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures




References
-
- Knutson V., Aleshin-Guendel S., Karlinsky A., Msemburi W., Wakefield J. World Health Organization; 2022. Estimating global and country-specific excess mortality during the COVID-19 pandemic.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
