

Impact of work schedules of senior resident physicians on patient and resident physician safety: nationwide, prospective cohort study
- PMID: 37303489
- PMCID: PMC10254593
- DOI: 10.1136/bmjmed-2022-000320
Impact of work schedules of senior resident physicians on patient and resident physician safety: nationwide, prospective cohort study
Abstract
Objective: To determine whether long weekly work hours and shifts of extended duration (≥24 hours) are associated with adverse patient and physician safety outcomes in more senior resident physicians (postgraduate year 2 and above; PGY2+).
Design: Nationwide, prospective cohort study.
Setting: United States, conducted over eight academic years (2002-07, 2014-17).
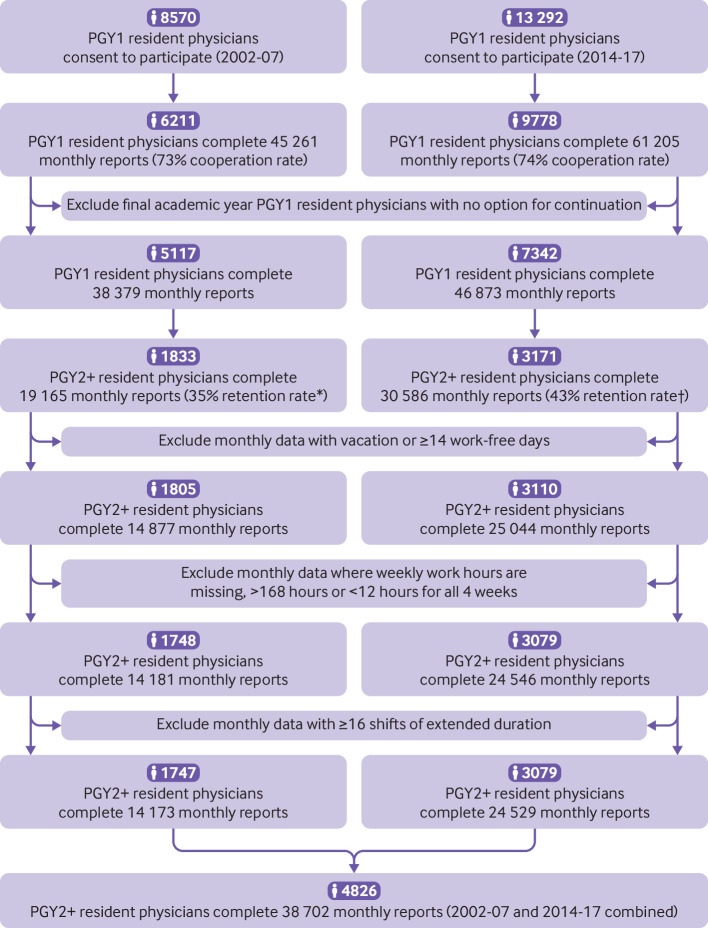
Participants: 4826 PGY2+ resident physicians who completed 38 702 monthly web based reports of their work hours and patient and resident safety outcomes.
Main outcome measures: Patient safety outcomes included medical errors, preventable adverse events, and fatal preventable adverse events. Resident physician health and safety outcomes included motor vehicle crashes, near miss crashes, occupational exposures to potentially contaminated blood or other bodily fluids, percutaneous injuries, and attentional failures. Data were analysed with mixed effects regression models that accounted for dependence of repeated measures and controlled for potential confounders.
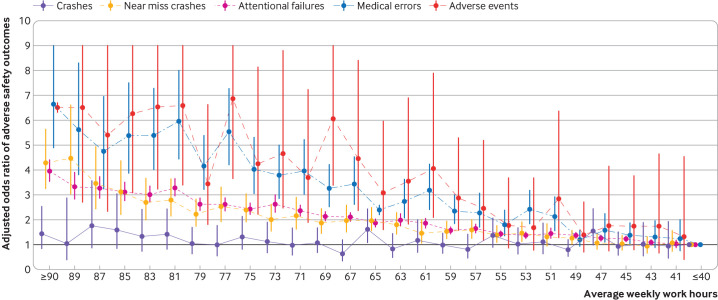
Results: Working more than 48 hours per week was associated with an increased risk of self-reported medical errors, preventable adverse events, and fatal preventable adverse events as well as near miss crashes, occupational exposures, percutaneous injuries, and attentional failures (all P<0.001). Working between 60 and 70 hours per week was associated with a more than twice the risk of a medical error (odds ratio 2.36, 95% confidence interval 2.01 to 2.78) and almost three times the risk of preventable adverse events (2.93, 2.04 to 4.23) and fatal preventable adverse events (2.75, 1.23 to 6.12). Working one or more shifts of extended duration in a month while averaging no more than 80 weekly work hours was associated with an 84% increased risk of medical errors (1.84, 1.66 to 2.03), a 51% increased risk of preventable adverse events (1.51, 1.20 to 1.90), and an 85% increased risk of fatal preventable adverse events (1.85, 1.05 to 3.26). Similarly, working one or more shifts of extended duration in a month while averaging no more than 80 weekly work hours also increased the risk of near miss crashes (1.47, 1.32 to 1.63) and occupational exposures (1.17, 1.02 to 1.33).
Conclusions: These results indicate that exceeding 48 weekly work hours or working shifts of extended duration endangers even experienced (ie, PGY2+) resident physicians and their patients. These data suggest that regulatory bodies in the US and elsewhere should consider lowering weekly work hour limits, as the European Union has done, and eliminating shifts of extended duration to protect the more than 150 000 physicians training in the US and their patients.
Keywords: Occupational health; Sleep medicine specialty.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from National Institute for Occupational Safety & Health (NIOSH) within the US Centers for Disease Control and the Agency for Healthcare Research and Quality for the submitted work. LKB reports support from NIOSH, National Heart, Lung, and Blood Institute (NHLBI), Puget Sound Pilots and Delta Airlines, through Brigham and Women’s Hospital and Brigham and Women’s Physician Organization and personal fees from Boston Children’s Hospital, University of Helsinki, and the AAA Foundation. MDW reports grant support from NIOSH, NHLBI, and US CDC, as well as consulting fees from the Fred Hutchinson Cancer Center, National Sleep Foundation, and University of Pittsburgh for activities outside the submitted work. JPS and SQ report no competing interests. CPL reports personal fees and other from I-PASS Patient Safety Institute, personal fees from Missouri Hospital Association/Executive Speakers Bureau, outside the submitted work; CPL has also received monetary awards, honorariums, and travel reimbursement from multiple academic and professional organisations for teaching and consulting on sleep deprivation, physician performance, handoffs, and safety, and has served as an expert witness in cases regarding patient safety and sleep deprivation. CAC reports grant support from NIOSH within the US CDC, Agency for HealthCare Research and Quality, and NHLBI. CAC serves as the incumbent of an endowed professorship provided to Harvard Medical School by Cephalon in 2004, which provided institutional support for this work. He has received additional support from Delta Airlines, Jazz Pharmaceuticals, Axome Therapeutics, Philips Respironics Puget Sound Pilots, Regeneron Pharmaceuticals and Sanofi SA, ResMed, Teva Pharmaceuticals Industries, and Vanda Pharmaceuticals. CAC receives royalty payments from Phillips Respironices on sales of the Actiwatch-2 and Actiwatch-Spectrum devices. He has received personal consultancy fees from With Deep and Vanda Pharmaceuticals. CAC has received honorariums from the Associated Professional Sleep Societies, Massachusetts Medical Society, and National Sleep Foundation and travel fees from Stanley Ho Medical Development Foundation and Associated Professional Sleep Societies. CAC has equity interest in Vanda Pharmaceuticals, With Deep, and Signos. CAC is an advisory board member for UK Biotechnology and Biological Sciences Research Council, Institute of Digital Media and Child Development and Klarman Family Foundation. CAC has received educational or research gifts (to Brigham and Women’s Hospital) from Johnson & Johnson, Mary Ann and Stanley Snider via Combined Jewish Philanthropies, Alexandra Drane, DR Capital Management, Harmony Biosciences, Vanda Pharmaceuticals, Eisai, Jazz Pharmaceuticals, Idorsia Pharmaceuticals, Sleep Number, Apnimed, Avadel Pharmaceuticals, Axome Therapeutics, Bryte Foundation, f.lux Software, Stuart F and Diana L Quan Charitable Fund, Casey Feldman Foundation, Roman Catholic Archdiocese of Boston, Summus, Takeda Pharmaceutical, Philips Respironics, Abbaszadeh Foundation, Sharon and John Loeb, CDC Foundation, US CDC, and ResMed. CAC’s interests were reviewed and are managed by the Brigham and Women’s Hospital and Mass General Brigham in accordance with their conflict-of-interest policies.
Figures
References
-
- Institute of Medicine (US) Committee on Optimizing Graduate Medical Trainee (Resident) Hours and Work Schedule to Improve Patient Safety . Resident duty hours. In: Ulmer C, Wolman DM, Johns MME, eds. Enhancing sleep, supervision, and safety. Washington, D.C: The National Academies Press, 2008: 1–322. - PubMed
-
- Accreditation Council for Graduate Medical Education . Common program requirements; 2010.
-
- Miettinen OS. Theoretical epidemiology: principles of occurrence research in medicine. New York: Wiley, 1985.
-
- Association of American Medical Colleges . Table B3. Number of active residents, by type of medical school, GME specialty, and sex. 2019. Available: https://www.aamc.org/data-reports/students-residents/interactive-data/re... [Accessed 14 Jul 2002].
Grants and funding
LinkOut - more resources
Full Text Sources