

Nucleoside/nucleotide reverse transcriptase inhibitor sparing regimen with once daily integrase inhibitor plus boosted darunavir is non-inferior to standard of care in virologically-suppressed children and adolescents living with HIV - Week 48 results of the randomised SMILE Penta-17-ANRS 152 clinical trial
- PMID: 37304494
- PMCID: PMC10251070
- DOI: 10.1016/j.eclinm.2023.102025
Nucleoside/nucleotide reverse transcriptase inhibitor sparing regimen with once daily integrase inhibitor plus boosted darunavir is non-inferior to standard of care in virologically-suppressed children and adolescents living with HIV - Week 48 results of the randomised SMILE Penta-17-ANRS 152 clinical trial
Abstract
Background: Integrase inhibitor (INSTI) with boosted darunavir (DRV/r), a regimen with a high-resistance barrier, avoiding NRTI toxicities, might be a switching option in children living with HIV (CLWHIV).
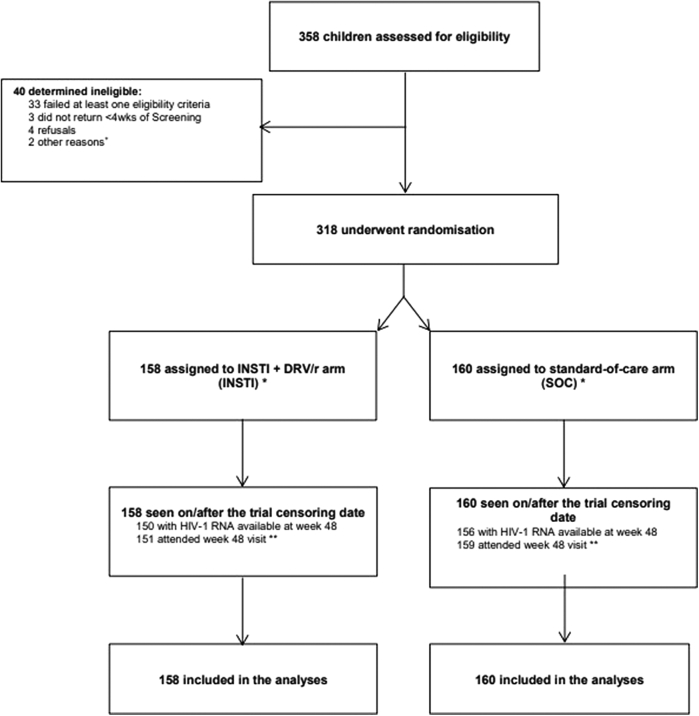
Methods: SMILE is a randomised non-inferiority trial evaluating safety and antiviral efficacy of once-daily INSTI + DRV/r vs. continuing on current standard-of-care (SOC) triple ART (2NRTI + boosted PI/NNRTI) in virologically-suppressed CLWHIV aged 6-18 years. The primary outcome is the proportion with confirmed HIV-RNA ≥50 copies/mL by week 48, estimated by Kaplan-Meier method. Non-inferiority margin was 10%. Registration number for SMILE are: ISRCTN11193709, NCT #: NCT02383108.
Findings: Between 10th June 2016 and 30th August 2019, 318 participants were enrolled from Africa 53%, Europe 24%, Thailand 15% and Latin America 8%, 158 INSTI + DRV/r [153 Dolutegravir (DTG); 5 Elvitegravir (EVG)], 160 SOC. Median (range) age was 14.7 years (7.6-18.0); CD4 count 782 cells/mm3 (227-1647); 61% female. Median follow-up was 64.3 weeks with no loss to follow-up. By 48 weeks, 8 INSTI + DRV/r vs. 12 SOC had confirmed HIV-RNA ≥50 copies/mL; difference (INSTI + DRV/r-SOC) -2.5% (95% CI: -7.6, 2.5%), showing non-inferiority. No major PI or INSTI resistance mutations were observed. There were no differences in safety between arms. By week 48, difference (INSTI + DRV/r-SOC) in mean CD4 count change from baseline was -48.3 cells/mm3 (95% CI: -93.4, -3.2; p = 0.036). Difference (INSTI + DRV/r-SOC) in mean HDL change from baseline was -4.1 mg/dL (95% CI: -6.7, -1.4; p = 0.003). Weight and Body Mass Index (BMI) increased more in INSTI + DRV/r than SOC [difference: 1.97 kg (95% CI: 1.1, 2.9; p < 0.001), 0.66 kg/m2 (95% CI: 0.3, 1.0; p < 0.001)].
Interpretation: In virologically-suppressed children, switching to INSTI + DRV/r was non-inferior virologically, with similar safety profile, to continuing SOC. Small but significant differences in CD4, HDL-cholesterol, weight and BMI were observed between INSTI + DRV/r vs. SOC although clinical relevance needs further investigation. SMILE data corroborate adult findings and provide evidence for this NRTI-sparing regimen for children and adolescents.
Funding: Fondazione Penta Onlus, Gilead, Janssen, INSERM/ANRS and UK MRC. ViiV-Healthcare provided Dolutegravir.
Keywords: Adolescents; Children; Darunavir; Dolutegravir; Dual therapy; HIV; Maintenance; Paediatrics; Randomised; Simplification; Virological suppressed.
© 2023 The Authors.
Conflict of interest statement
ACom, YS, YR and ACoe declare that their institution Inserm received a grant for the trial through PENTA Foundation “agreement PENTA-Inserm” started 14th September 2014 and declare support for scientific meetings from PENTA Foundation. AVi declares funding given from PENTA Foundation to her institution for the conduct of the study. ABab declares a grant from Medical Research Council, UKRI to his Institution. PA and ADK declare sponsored study materials and participant recruitment costs from PENTA foundation. PA, ADK and CG declare a research grant for part of the study from Gilead and funded drug supply for the study from ViiV Healthcare. NPR declares a financial support for the research paid to her institution from PENTA Foundation and from Merck. NPR declares that her institution receives the drugs for the study from PENTA Foundation. NPR declares a support for attending ID week in 2022 from AstraZeneca. All other authors declare no competing interests.
Figures
References
-
- Guidelines for the use of antiretroviral agents in pediatric HIV infection. Developed by the HHS panel on antiretroviral therapy and medical management of HIV-infected children-A working group of the office of AIDS research advisory Council (OARAC) http://aidsinfo.nih.gov/guidelines Access december 2021.
-
- Updated recommendations on HIV prevention, infant diagnosis, antiretroviral initiation and monitoring: march 2021. World Health Organization; Geneva: 2021. - PubMed
-
- Food Drug Administration Center for Drugs Evaluation Research . FDA; Maryland, USA: 2015. Human immunodeficiency virus-1 infection: developing antiretroviral drugs for treatment - guidance for industry; p. 9.
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
