

Urinary tract infection in children: A narrative review of clinical practice guidelines
- PMID: 37304508
- PMCID: PMC10252788
- DOI: 10.4103/ua.ua_147_22
Urinary tract infection in children: A narrative review of clinical practice guidelines
Abstract
Background: Urinary tract infection (UTI) has been a major burden on the community and the health-care systems all over the globe. It is the most common cause of bacterial infection in the pediatric age group, with an annual incidence of 3%. The aim of this study is to review and summarize all available guidelines on the diagnosis and management of children with UTI.
Materials and methods: This is a narrative review of the management of children with a UTI. All biomedical databases were searched, and any guidelines published from 2000 to 2022 were retrieved, reviewed, and evaluated to be included in the summary statements. The sections of the articles were formulated according to the availability of information in the included guidelines.
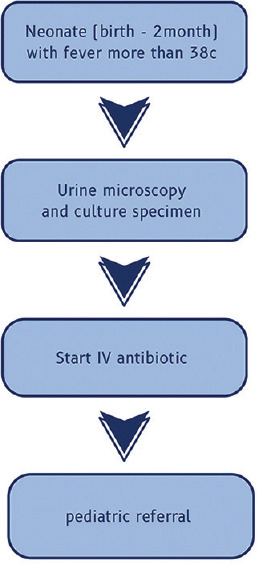
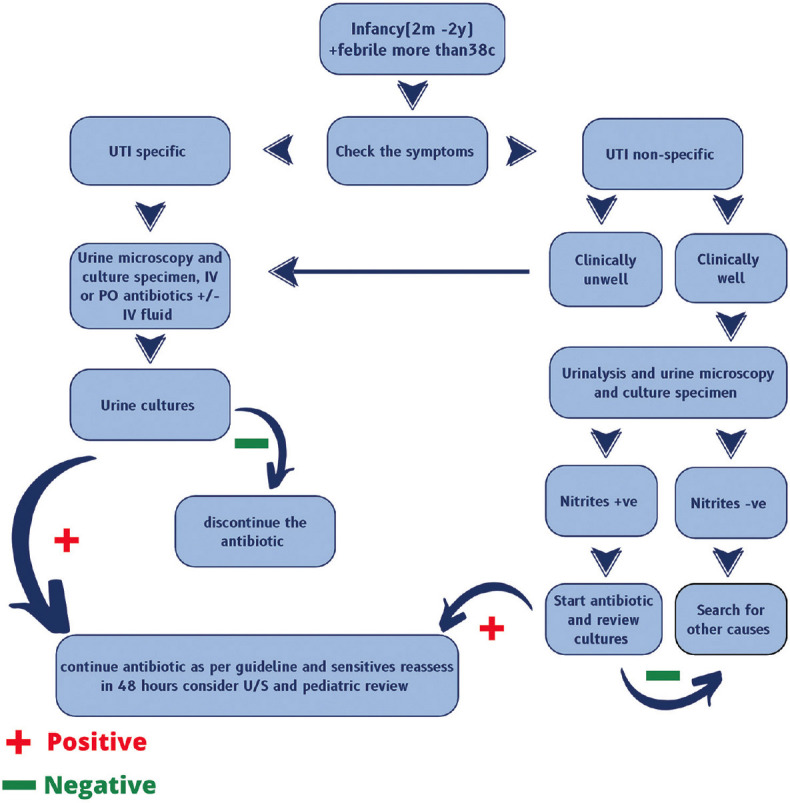
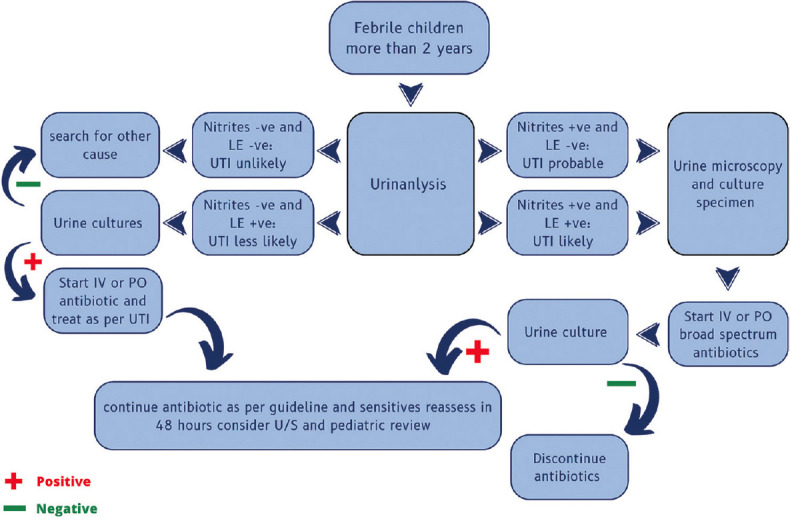
Results: UTI diagnoses are based on positive urine culture from a specimen of urine obtained through catheterization or suprapubic aspiration, and diagnoses cannot be established on the bases of urine collected from a bag. The criteria for diagnosing UTI are based on the presence of at least 50,000 colony-forming units per milliliter of a uropathogen. Upon confirmation of UTI, the clinician should instruct parents to seek rapid medical assessment (ideally within 48 h) of future febrile disease to ensure that frequent infections can be detected and treated immediately. The choice of therapy depends on several factors, including the age of the child, underlying medical problems, the severity of the disease, the ability to tolerate oral medications, and most importantly local patterns of uropathogens resistance. Initial antibiotic choice of treatment should be according to the sensitivity results or known pathogens patterns with comparable efficacy of oral and parenteral route, for 7 days to 14 days duration. Renal and bladder ultrasonography is the investigation of choice for febrile UTI, and voiding cystourethrography should not be performed routinely unless indicated.
Conclusion: This review summarizes all the recommendations related to UTIs in the pediatric population. Due to the lack of appropriate data, further high-quality studies are required to improve the level and strength of recommendations in the future.
Keywords: Children; clinical practice guidelines; cystitis; pediatric; pyelonephritis; urinary tract infection; vesicoureteric reflux.
Copyright: © 2023 Urology Annals.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: Ameta-analysis. Pediatr Infect Dis J. 2008;27:302–8. - PubMed
-
- Beetz R. May we go on with antibacterial prophylaxis for urinary tract infections? Pediatr Nephrol. 2006;21:5–13. - PubMed
-
- Desai DJ, Gilbert B, McBride CA. Paediatric urinary tract infections: Diagnosis and treatment. Aust Fam Physician. 2016;45:558–63. - PubMed
-
- Hoberman A, Chao HP, Keller DM, Hickey R, Davis HW, Ellis D. Prevalence of urinary tract infection in febrile infants. J Pediatr. 1993;123:17–23. - PubMed
Publication types
LinkOut - more resources
Full Text Sources