

Valve-sparing root replacement-reimplantation technique
- PMID: 37304699
- PMCID: PMC10248919
- DOI: 10.21037/acs-2022-avs1-12
Valve-sparing root replacement-reimplantation technique
Abstract
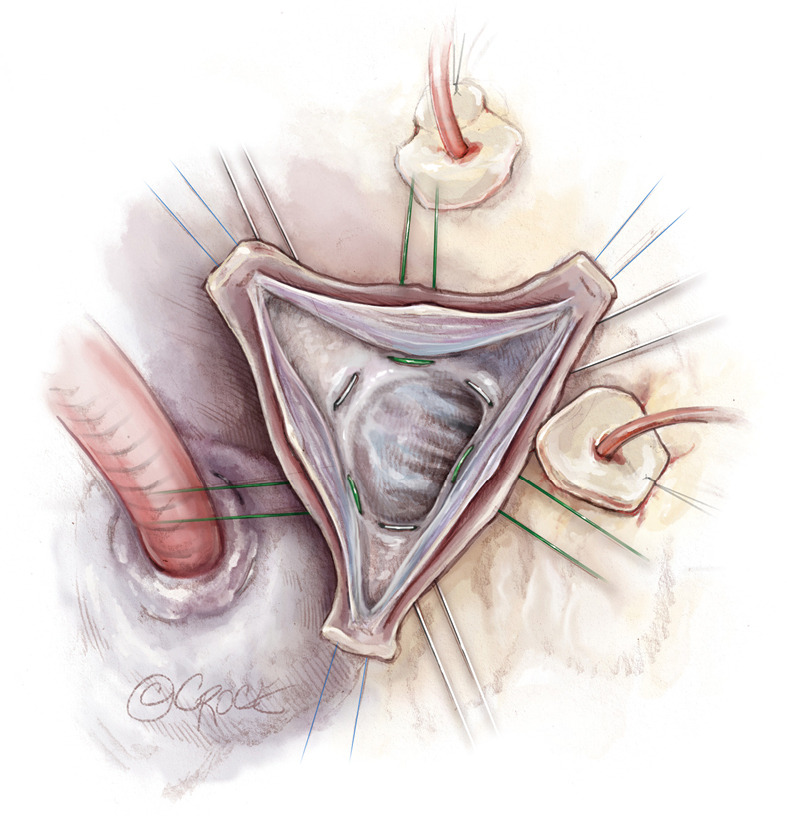
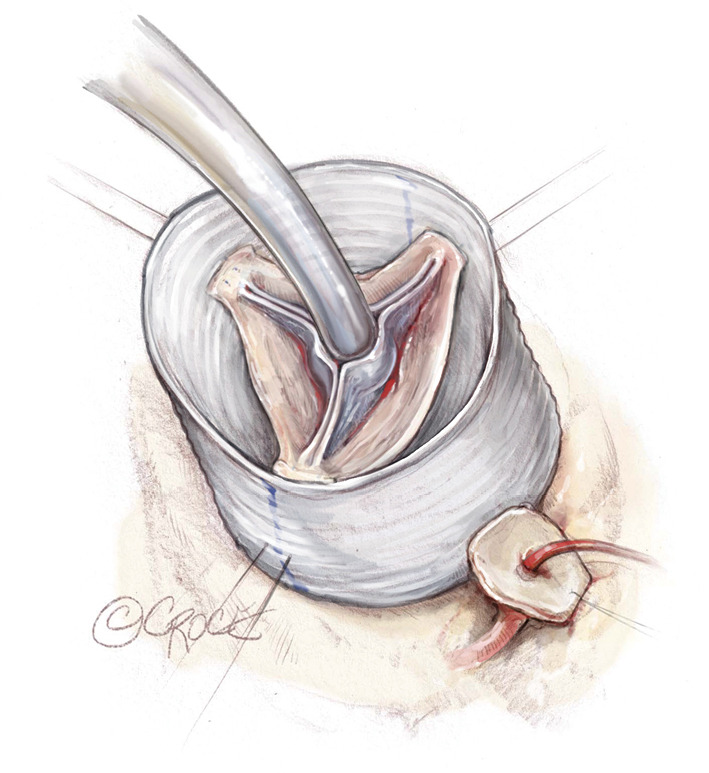
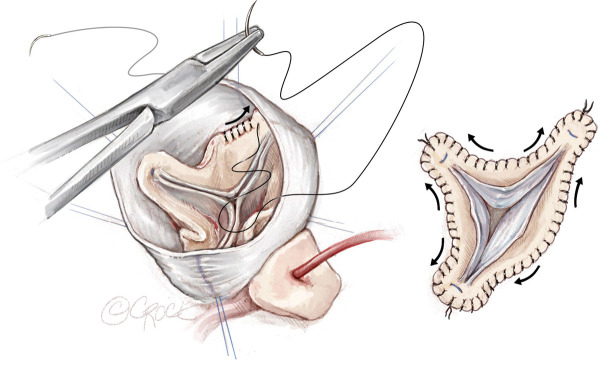
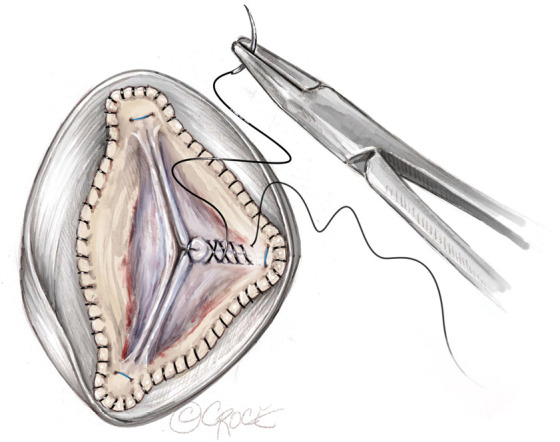
The first valve sparing root replacement (VSRR) was first described over thirty years ago. Reimplantation is favored at our institution to provide maximum annular support in the setting of annuloaortic ectasia. Multiple iterations for this operation have been reported. Surgical intervention varies in terms of graft sizing, the number and method of inflow suture placement, strategy for annular plication and stabilization, and finally choice of graft type. Our specific technique has evolved over the last eighteen years and the current approach is to use a larger straight graft loosely based on the original Feindel-David formula, six inflow sutures to anchor the graft, and some degree of annular plication with annular stabilization. The long-term results for both trileaflet and bicuspid valves are associated with a low reintervention rate. Herein we provide a clear outline for our specific approach to the reimplantation technique.
Keywords: Bicuspid aortic valve (BAV); aortic annuloplasty; aortic valve regurgitation; reimplantation technique; valve-sparing root replacement.
2023 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources