

Expanding epidemic of recently acquired HCV in HIV-coinfected patients over a period of 10 years
- PMID: 37305441
- PMCID: PMC10250927
- DOI: 10.1016/j.jhepr.2023.100701
Expanding epidemic of recently acquired HCV in HIV-coinfected patients over a period of 10 years
Abstract
Background & aims: Ongoing transmission of HCV infections is associated with risk factors such as drug injection, needlestick injuries, and men who have sex with men (MSM). Ways of transmission, the course of acute infection, changes of virologic features, and incidence over time are not well known.
Methods: Over a period of 10 years, n = 161 patients with recently acquired HCV infection (RAHC) (median follow-up 6.8 years) were prospectively enrolled. NS5B sequencing was performed to re-evaluate the HCV genotype (GT) and for phylogenetic analyses.
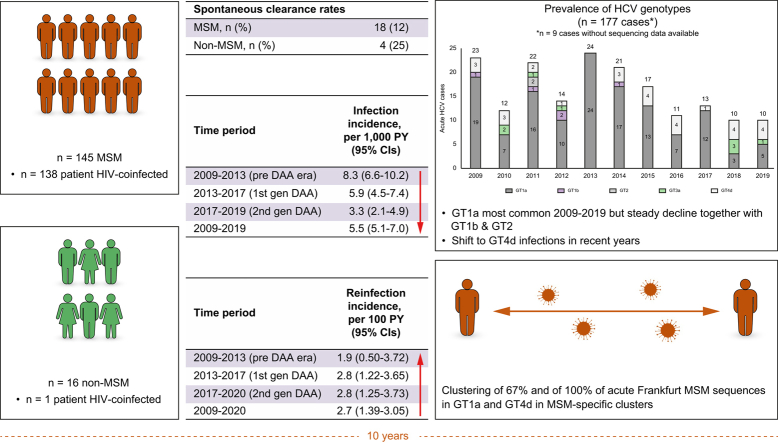
Results: Patients with RAHC were mainly male (92.5%), MSM (90.1%), and HIV-coinfected (86.3%). Transmission risk factors for MSM and non-MSM were sexual risk behaviour (100 and 6.3%, respectively), injection drug use (9.7 and 37.5%, respectively), and nasal drug use (15.2 and 0%, respectively). Spontaneous and interferon- or direct-acting antiviral-based clearance rates were 13.6, 84.3 and 93.4%, respectively. Mean RAHC declined from 19.8 in the first to 13.2 in the past five study years. Although the majority of infections was caused by HCV GT1a, the frequency of HCV GT4d and slightly HCV GT3a increased over time. No relevant clustering of HCV isolates was observed in non-MSM. However, 45% of HCV GT1a and 100% of HCV GT4d MSM cases clustered with MSM isolates from other countries. Travel-associated infections were supported by personal data in an MSM subgroup. No international clustering was detected in MSM with HCV GT1b or HCV GT3a.
Conclusions: RAHCs were mainly diagnosed in HIV-coinfected MSM patients and were associated with sexual risk behaviour. Spontaneous clearance rates were low, and phylogenetic clusters were observed in the majority of patients.
Impact and implications: We evaluated the occurrence and transmission of recently acquired HCV infections (RAHCs) over a period of 10 years. Our data demonstrate that the presence of RAHC was mainly found in HIV-coinfected MSM, with internationally connected transmission networks being observed in the majority of patients. Spontaneous clearance rates were low, and reinfection rates increased mainly driven by a small subset of MSM patients with high-risk behaviour.
Keywords: Acute HCV infection; HCV; HIV coinfection; MSM; NS5B phylogeny.
© 2023 The Authors.
Conflict of interest statement
CG has received speaking and/or consulting fees from AbbVie and Gilead. FF has received travel support from Abbvie and Novartis, speaker fees from Abbvie and MSD, and consulting fees from Fresenius and Ibsen. GD has received speaking and/or consulting fees from AbbVie and Gilead. SZ has received speaking and/or consulting fees from Abbvie, BMS, Gilead, Janssen, and Merck/MSD. JD has received research support from Gilead. CZ has received speaking and/or consulting fees from Abbvie, BMS, Gilead, and Merck/MSD, and research support from Abbvie and Gilead. LH, TL, CS, GK, PG, MB, KHP, AM, NW, NF, EH, and NB have no conflicts to disclose. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



 ) non-MSM, Frankfurt, Germany; (
) non-MSM, Frankfurt, Germany; ( ) MSM, Frankfurt, Germany; (red) MSM (published sequences), Germany; (dark blue) MSM (published sequences), UK; (orange) MSM (published sequences), Netherlands; (grey) MSM (published sequences), Switzerland; (yellow) MSM (published sequences), Spain; (light blue) MSM (published sequences), USA; (pink) MSM (published sequences), Canada; (purple) MSM (published sequences), Australia; (green) MSM (published sequences), France. GT, genotype.
) MSM, Frankfurt, Germany; (red) MSM (published sequences), Germany; (dark blue) MSM (published sequences), UK; (orange) MSM (published sequences), Netherlands; (grey) MSM (published sequences), Switzerland; (yellow) MSM (published sequences), Spain; (light blue) MSM (published sequences), USA; (pink) MSM (published sequences), Canada; (purple) MSM (published sequences), Australia; (green) MSM (published sequences), France. GT, genotype. ) non-MSM, Frankfurt, Germany; () MSM, Frankfurt, Germany; (red) MSM (published sequences), Germany; (dark blue) MSM (published sequences), UK; (orange) MSM (published sequences), Netherlands; (grey) MSM (published sequences), Switzerland; (yellow) MSM (published sequences), Spain; (light blue) MSM (published sequences), USA; (pink) MSM (published sequences), Canada; (purple) MSM (published sequences), Australia; (green) MSM (published sequences), France. GT, genotype.
) non-MSM, Frankfurt, Germany; () MSM, Frankfurt, Germany; (red) MSM (published sequences), Germany; (dark blue) MSM (published sequences), UK; (orange) MSM (published sequences), Netherlands; (grey) MSM (published sequences), Switzerland; (yellow) MSM (published sequences), Spain; (light blue) MSM (published sequences), USA; (pink) MSM (published sequences), Canada; (purple) MSM (published sequences), Australia; (green) MSM (published sequences), France. GT, genotype.References
-
- Price J.C., Brandman D. Updated hepatitis C virus screening recommendation – a step forward. JAMA Intern Med. 2020;180:637–639. - PubMed
-
- Hoornenborg E., Achterbergh R.C.A., Schim van der Loeff M.F., Davidovich U., Hogewoning A., de Vries H.J.C., et al. MSM starting preexposure prophylaxis are at risk of hepatitis C virus infection. AIDS. 2017;31:1603–1610. - PubMed
-
- Deterding K., Spinner C.D., Schott E., Welzel T.M., Gerken G., Klinker H., et al. Ledipasvir plus sofosbuvir fixed-dose combination for 6 weeks in patients with acute hepatitis C virus genotype 1 monoinfection (HepNet Acute HCV IV): an open-label, single-arm, phase 2 study. Lancet Infect Dis. 2017;17:215–222. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
