

Cardiovascular Burden of Narcolepsy Disease (CV-BOND): a real-world evidence study
- PMID: 37305967
- PMCID: PMC10566243
- DOI: 10.1093/sleep/zsad161
Cardiovascular Burden of Narcolepsy Disease (CV-BOND): a real-world evidence study
Abstract
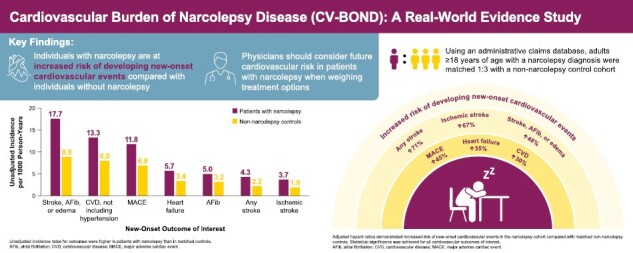
Study objectives: Narcolepsy is associated with cardiovascular risk factors; however, the risk of new-onset cardiovascular events in this population is unknown. This real-world study evaluated the excess risk of new-onset cardiovascular events in U.S. adults with narcolepsy.
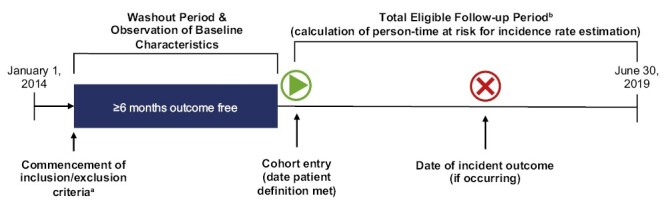
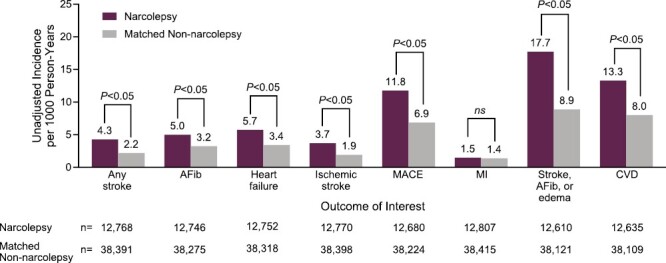
Methods: A retrospective cohort study using IBM MarketScan administrative claims data (2014-2019) was conducted. A narcolepsy cohort, comprising adults (≥18 years) with at least two outpatient claims containing a narcolepsy diagnosis, of which at least one was non-diagnostic, was matched to a non-narcolepsy control cohort (1:3) based on cohort entry date, age, sex, geographic region, and insurance type. The relative risk of new-onset cardiovascular events was estimated using a multivariable Cox proportional hazards model to compute adjusted hazard ratios (HRs) and 95% confidence intervals (CIs).
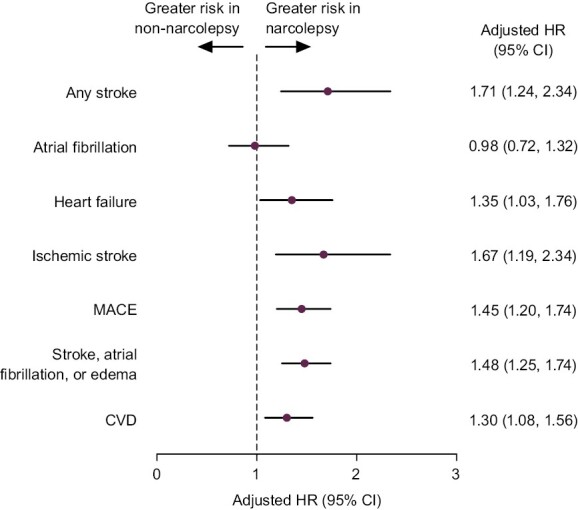
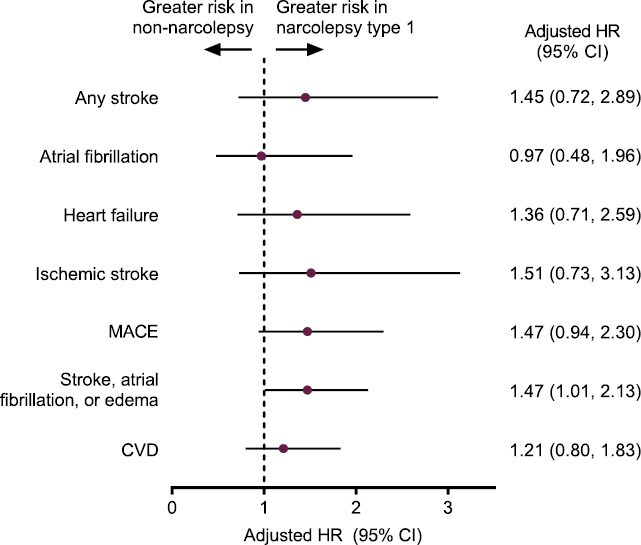
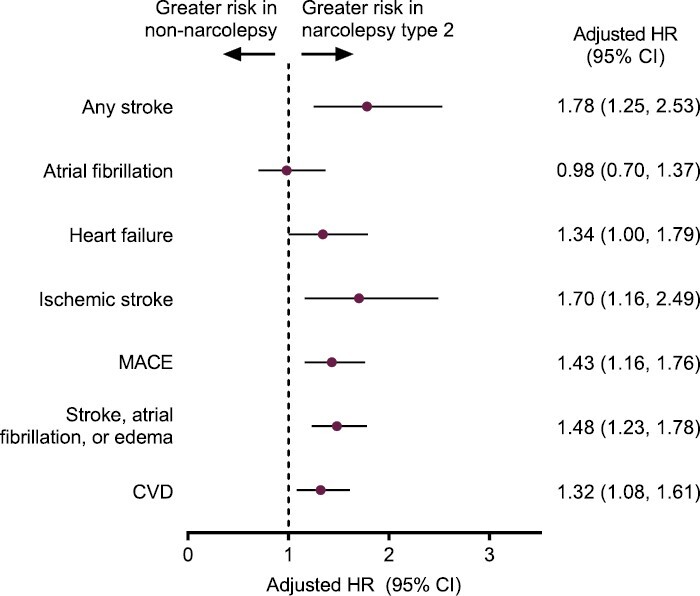
Results: The narcolepsy and matched non-narcolepsy control cohorts included 12 816 and 38 441 individuals, respectively. At baseline, cohort demographics were generally similar; however, patients with narcolepsy had more comorbidities. In adjusted analyses, the risk of new-onset cardiovascular events was higher in the narcolepsy cohort compared with the control cohort: any stroke (HR [95% CI], 1.71 [1.24, 2.34]); heart failure (1.35 [1.03, 1.76]); ischemic stroke (1.67 [1.19, 2.34]); major adverse cardiac event (1.45 [1.20, 1.74]); grouped instances of stroke, atrial fibrillation, or edema (1.48 [1.25, 1.74]); and cardiovascular disease (1.30 [1.08, 1.56]).
Conclusion: Individuals with narcolepsy are at increased risk of new-onset cardiovascular events compared with individuals without narcolepsy. Physicians should consider cardiovascular risk in patients with narcolepsy when weighing treatment options.
Keywords: cardiovascular; comorbidities; narcolepsy; stroke.
© The Author(s) 2023. Published by Oxford University Press on behalf of Sleep Research Society.
Figures
Comment in
-
Cardiovascular burden of narcolepsy: what have we learned and what do we still need to know?Sleep. 2023 Oct 11;46(10):zsad213. doi: 10.1093/sleep/zsad213. Sleep. 2023. PMID: 37586395 No abstract available.
References
-
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
-
- Dauvilliers Y, et al. . Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology. 2001;57(11):2029–2033. - PubMed
