

Pain, function and quality of life are impaired in adults undergoing periacetabular osteotomy (PAO) for hip dysplasia: a systematic review and meta-analysis
- PMID: 37306161
- PMCID: PMC10787396
- DOI: 10.1177/11207000231179610
Pain, function and quality of life are impaired in adults undergoing periacetabular osteotomy (PAO) for hip dysplasia: a systematic review and meta-analysis
Abstract
Background: Hip dysplasia is a common condition in active adults with hip pain that can lead to joint degeneration. Periacetabular osteotomy (PAO) is a common surgical treatment for hip dysplasia. The effect of this surgery on pain, function and quality of life (QOL) has not been systematically analysed.
Purpose: In adults with hip dysplasia: (1) evaluate differences in pain, function and QOL in those undergoing PAO and healthy controls; (2) evaluate pre- to post-PAO changes in pain, function and QOL; (3) evaluate differences in pain, function and QOL in those with mild versus severe dysplasia, undergoing PAO; and (4) evaluate differences in pain, function and QOL in those having primary PAO versus those with previous hip arthroscopy.
Methods: A comprehensive, reproducible search strategy was performed on 5 different databases. We included studies that assessed pain, function and QOL in adults undergoing PAO for hip dysplasia, using hip-specific patient reported outcomes measures.
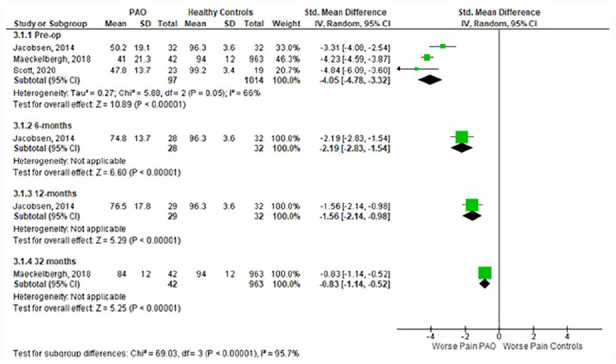
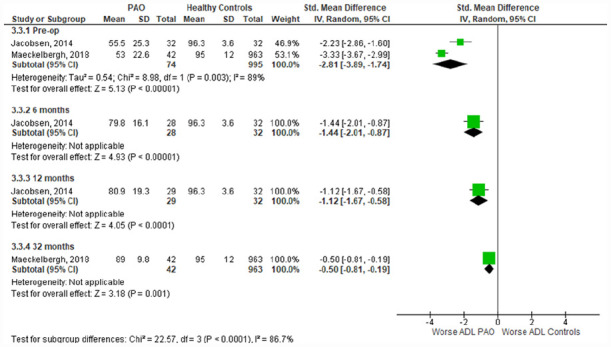
Results: From 5017 titles and abstracts screened, 62 studies were included. Meta-analysis showed PAO patients had worse outcomes pre- and post-PAO compared to healthy participants. Specifically, pain (standardised mean difference [SMD] 95% confidence interval [CI]): -4.05; -4.78 to -3.32), function (-2.81; -3.89 to -1.74), and QOL (-4.10; -4.43 to -3.77) were significantly poorer preoperatively.Meta-analysis found patients experienced improvements following PAO. Pain improved from pre-surgery to 1-year (standardised paired difference [SPD] 1.35; 95% CI, 1.02-1.67) and 2 years postoperatively (1.35; 1.16-1.54). For function, the activities of daily living scores at 1 year (1.22; 1.09-1.35) and 2 years (1.06; 0.9-1.22) and QOL at 1 year (1.36; 1.22-1.5) and 2 years (1.3; 1.1-1.5) all improved. No difference was found between patients undergoing PAO with mild versus severe dysplasia.
Conclusions: Before undergoing PAO surgery, adults with hip dysplasia have worse levels of pain, function and QOL compared to healthy participants. These levels improve following PAO, but do not reach the same level as their healthy participants.
Registration: PROSPERO (CRD42020144748).
Keywords: Developmental dysplasia of the hip; hip dysplasia; hip joint; periacetabular osteotomy; rehabilitation.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Gala L, Clohisy JC, Beaulé PE. Hip dysplasia in the young adult. J Bone Joint Surg Am 2016; 98: 63–73. - PubMed
-
- Schmitz MR, Murtha AS, Clohisy JC, et al. Developmental dysplasia of the hip in adolescents and young adults. J Am Acad Orthop Surg 2020; 28: 91–101. - PubMed
-
- Clohisy JC, Dobson MA, Robison JF, et al. Radiographic structural abnormalities associated with premature, natural hip-joint failure. J Bone Joint Surg Am 2011; 93(Suppl. 2): 3–9. - PubMed
-
- Cooperman D. What is the evidence to support acetabular dysplasia as a cause of osteoarthritis? J Pediatr Orthop 2013; 33(Suppl. 1): S2–S7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
