

Comparison of positive pressure extubation with traditional extubation in critically ill patients - a randomised control study
- PMID: 37306270
- PMCID: PMC10156539
- DOI: 10.5114/ait.2023.125584
Comparison of positive pressure extubation with traditional extubation in critically ill patients - a randomised control study
Abstract
Background: Two extubation methods are commonly used in the intensive care unit (ICU): the traditional method with endotracheal suctioning and the positive- pressure method without suctioning. Better physiological outcomes were found in lab studies using the latter, as the air passing between the endotracheal tube and the larynx pushes out the collected subglottic secretions, which can be suctioned.
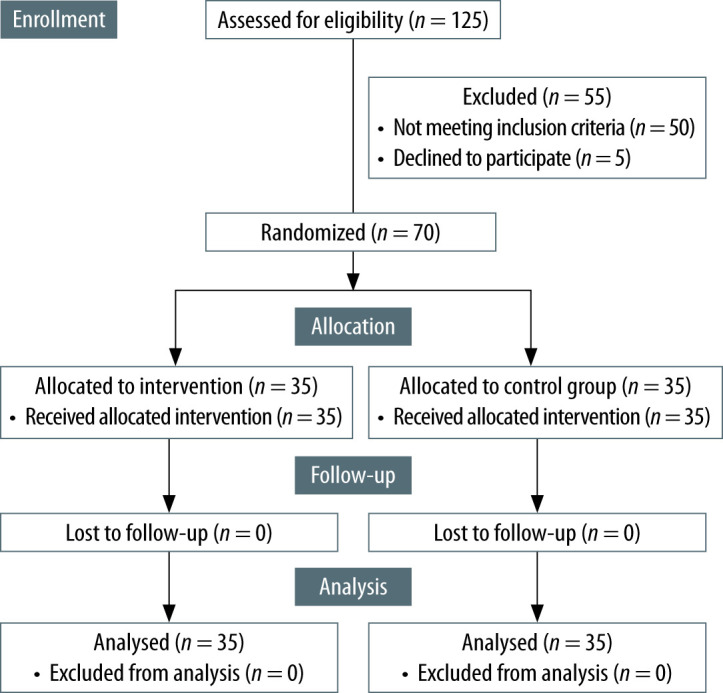
Methods: 70 mechanically ventilated patients in a tertiary ICU were randomised into 2 groups of 35 patients each. At the end of the spontaneous breathing trial (SBT), the positive pressure extubation (PPE) group was given a pressure support of 15 cm H 2 O and a positive end expiratory pressure of 10 cm H 2 O for 5 minutes while the other group (traditional extubation - TE) was extubated directly. We compared the lung ultrasound scores (LUS), chest X-ray findings, alveolar arterial oxygen gradient changes, adverse clinical events, ICU-free days and reintubation rates between the two groups.
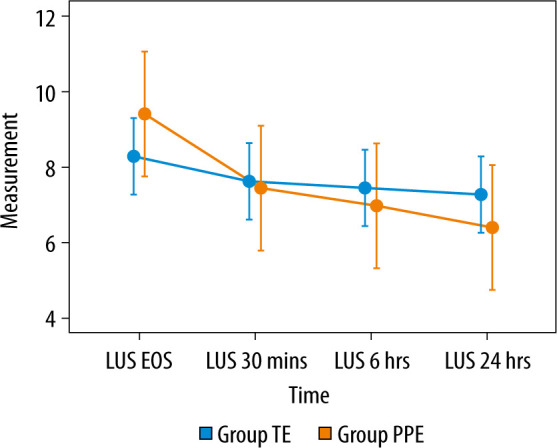
Results: Median LUS at the end of the SBT was similar between the two groups. However, the median post-extubation LUS at 30 minutes, 6 hours, 24 hours in the PPE group [5 (4-8) ( P = 0.04), 5 (3-8) ( P = 0.02), 4 (3-7) ( P = 0.02), respectively] were significantly lower compared to the TE group [6 (6-8), 6 (5-7.5), 6 (5-7.5), respectively]. There was a persistent lowering of the scores even at the end of 24 hours in the PPE group, while the percentage of patients without adverse clinical events was significantly higher (80% vs. 57.14%, P = 0.04).
Conclusions: The study shows that positive pressure extubation is a safe procedure which improves aeration and reduces adverse events.
Keywords: lung ultrasound; positive pressure extubation; traditional extubation; mechanical ventilation.
Conflict of interest statement
none.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous