

Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm
- PMID: 37306629
- PMCID: PMC10723864
- DOI: 10.1097/CORR.0000000000002706
Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm
Erratum in
-
Erratum to: Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2025 Jun 1;483(6):1175-1176. doi: 10.1097/CORR.0000000000003513. Epub 2025 May 22. Clin Orthop Relat Res. 2025. PMID: 40460329 No abstract available.
Abstract
Background: The Skeletal Oncology Research Group machine-learning algorithm (SORG-MLA) was developed to predict the survival of patients with spinal metastasis. The algorithm was successfully tested in five international institutions using 1101 patients from different continents. The incorporation of 18 prognostic factors strengthens its predictive ability but limits its clinical utility because some prognostic factors might not be clinically available when a clinician wishes to make a prediction.
Questions/purposes: We performed this study to (1) evaluate the SORG-MLA's performance with data and (2) develop an internet-based application to impute the missing data.
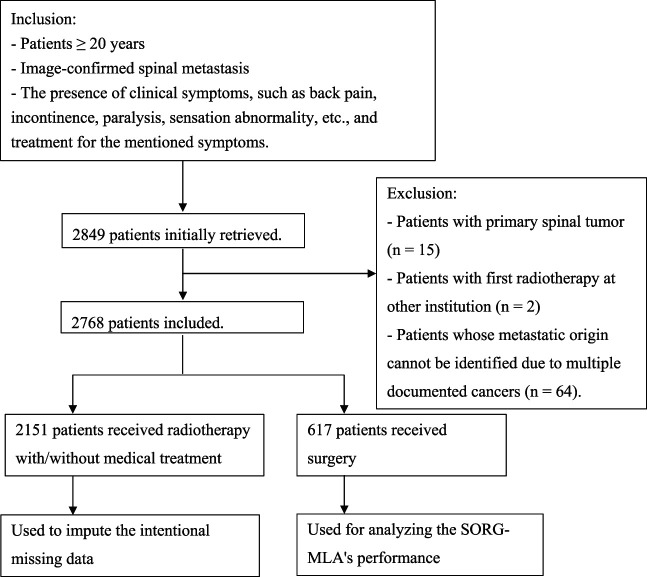
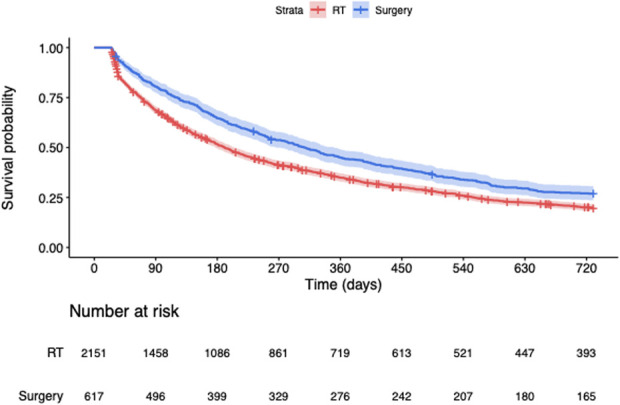
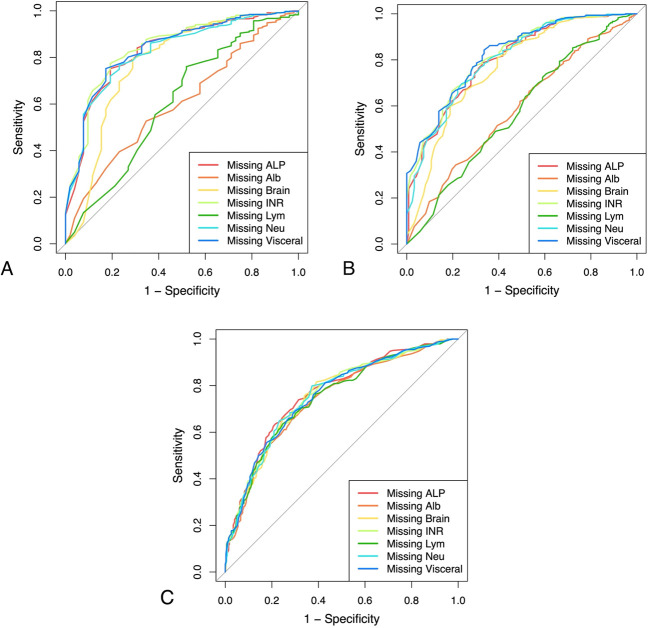
Methods: A total of 2768 patients were included in this study. The data of 617 patients who were treated surgically were intentionally erased, and the data of the other 2151 patients who were treated with radiotherapy and medical treatment were used to impute the artificially missing data. Compared with those who were treated nonsurgically, patients undergoing surgery were younger (median 59 years [IQR 51 to 67 years] versus median 62 years [IQR 53 to 71 years]) and had a higher proportion of patients with at least three spinal metastatic levels (77% [474 of 617] versus 72% [1547 of 2151]), more neurologic deficit (normal American Spinal Injury Association [E] 68% [301 of 443] versus 79% [1227 of 1561]), higher BMI (23 kg/m 2 [IQR 20 to 25 kg/m 2 ] versus 22 kg/m 2 [IQR 20 to 25 kg/m 2 ]), higher platelet count (240 × 10 3 /µL [IQR 173 to 327 × 10 3 /µL] versus 227 × 10 3 /µL [IQR 165 to 302 × 10 3 /µL], higher lymphocyte count (15 × 10 3 /µL [IQR 9 to 21× 10 3 /µL] versus 14 × 10 3 /µL [IQR 8 to 21 × 10 3 /µL]), lower serum creatinine level (0.7 mg/dL [IQR 0.6 to 0.9 mg/dL] versus 0.8 mg/dL [IQR 0.6 to 1.0 mg/dL]), less previous systemic therapy (19% [115 of 617] versus 24% [526 of 2151]), fewer Charlson comorbidities other than cancer (28% [170 of 617] versus 36% [770 of 2151]), and longer median survival. The two patient groups did not differ in other regards. These findings aligned with our institutional philosophy of selecting patients for surgical intervention based on their level of favorable prognostic factors such as BMI or lymphocyte counts and lower levels of unfavorable prognostic factors such as white blood cell counts or serum creatinine level, as well as the degree of spinal instability and severity of neurologic deficits. This approach aims to identify patients with better survival outcomes and prioritize their surgical intervention accordingly. Seven factors (serum albumin and alkaline phosphatase levels, international normalized ratio, lymphocyte and neutrophil counts, and the presence of visceral or brain metastases) were considered possible missing items based on five previous validation studies and clinical experience. Artificially missing data were imputed using the missForest imputation technique, which was previously applied and successfully tested to fit the SORG-MLA in validation studies. Discrimination, calibration, overall performance, and decision curve analysis were applied to evaluate the SORG-MLA's performance. The discrimination ability was measured with an area under the receiver operating characteristic curve. It ranges from 0.5 to 1.0, with 0.5 indicating the worst discrimination and 1.0 indicating perfect discrimination. An area under the curve of 0.7 is considered clinically acceptable discrimination. Calibration refers to the agreement between the predicted outcomes and actual outcomes. An ideal calibration model will yield predicted survival rates that are congruent with the observed survival rates. The Brier score measures the squared difference between the actual outcome and predicted probability, which captures calibration and discrimination ability simultaneously. A Brier score of 0 indicates perfect prediction, whereas a Brier score of 1 indicates the poorest prediction. A decision curve analysis was performed for the 6-week, 90-day, and 1-year prediction models to evaluate their net benefit across different threshold probabilities. Using the results from our analysis, we developed an internet-based application that facilitates real-time data imputation for clinical decision-making at the point of care. This tool allows healthcare professionals to efficiently and effectively address missing data, ensuring that patient care remains optimal at all times.
Results: Generally, the SORG-MLA demonstrated good discriminatory ability, with areas under the curve greater than 0.7 in most cases, and good overall performance, with up to 25% improvement in Brier scores in the presence of one to three missing items. The only exceptions were albumin level and lymphocyte count, because the SORG-MLA's performance was reduced when these two items were missing, indicating that the SORG-MLA might be unreliable without these values. The model tended to underestimate the patient survival rate. As the number of missing items increased, the model's discriminatory ability was progressively impaired, and a marked underestimation of patient survival rates was observed. Specifically, when three items were missing, the number of actual survivors was up to 1.3 times greater than the number of expected survivors, while only 10% discrepancy was observed when only one item was missing. When either two or three items were omitted, the decision curves exhibited substantial overlap, indicating a lack of consistent disparities in performance. This finding suggests that the SORG-MLA consistently generates accurate predictions, regardless of the two or three items that are omitted. We developed an internet application ( https://sorg-spine-mets-missing-data-imputation.azurewebsites.net/ ) that allows the use of SORG-MLA with up to three missing items.
Conclusion: The SORG-MLA generally performed well in the presence of one to three missing items, except for serum albumin level and lymphocyte count (which are essential for adequate predictions, even using our modified version of the SORG-MLA). We recommend that future studies should develop prediction models that allow for their use when there are missing data, or provide a means to impute those missing data, because some data are not available at the time a clinical decision must be made.
Clinical relevance: The results suggested the algorithm could be helpful when a radiologic evaluation owing to a lengthy waiting period cannot be performed in time, especially in situations when an early operation could be beneficial. It could help orthopaedic surgeons to decide whether to intervene palliatively or extensively, even when the surgical indication is clear.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2024 Jan 1;482(1):158-160. doi: 10.1097/CORR.0000000000002782. Epub 2023 Jul 25. Clin Orthop Relat Res. 2024. PMID: 37493449 Free PMC article. No abstract available.
Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Are Current Survival Prediction Tools Useful When Treating Subsequent Skeletal-related Events From Bone Metastases?Clin Orthop Relat Res. 2024 Sep 1;482(9):1710-1721. doi: 10.1097/CORR.0000000000003030. Epub 2024 Mar 22. Clin Orthop Relat Res. 2024. PMID: 38517402
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
Cited by
-
Erratum to: Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2025 Jun 1;483(6):1175-1176. doi: 10.1097/CORR.0000000000003513. Epub 2025 May 22. Clin Orthop Relat Res. 2025. PMID: 40460329 No abstract available.
-
Predicting the prognosis of radical gastrectomy for patients with locally advanced gastric cancer after neoadjuvant chemotherapy using machine learning technology: a multicenter study in China.Surg Endosc. 2025 Aug;39(8):5152-5170. doi: 10.1007/s00464-025-11946-4. Epub 2025 Jul 9. Surg Endosc. 2025. PMID: 40634722
-
Artificial Intelligence in bone Metastases: A systematic review in guideline adherence of 92 studies.J Bone Oncol. 2025 Apr 24;52:100682. doi: 10.1016/j.jbo.2025.100682. eCollection 2025 Jun. J Bone Oncol. 2025. PMID: 40337637 Free PMC article. Review.
-
Is it feasible to develop a supervised learning algorithm incorporating spinopelvic mobility to predict impingement in patients undergoing total hip arthroplasty?Bone Jt Open. 2024 Aug 14;5(8):671-680. doi: 10.1302/2633-1462.58.BJO-2024-0020.R1. Bone Jt Open. 2024. PMID: 39139101 Free PMC article.
References
-
- Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950;3:74-85. - PubMed
-
- Bongers MER, Karhade AV, Villavieja J, et al. Does the SORG algorithm generalize to a contemporary cohort of patients with spinal metastases on external validation? Spine J. 2020;20:1646-1652. - PubMed
-
- Bouras T, Zairi F, Arikat A, Vieillard MH, Allaoui M, Assaker R. Decision making for the surgical treatment of vertebral metastases among patients with short predicted survival. World Neurosurg. 2018;111:e573-e580. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
