

Evaluation of Oseltamivir Used to Prevent Hospitalization in Outpatients With Influenza: A Systematic Review and Meta-Analysis
- PMID: 37306992
- PMCID: PMC10262060
- DOI: 10.1001/jamainternmed.2023.0699
Evaluation of Oseltamivir Used to Prevent Hospitalization in Outpatients With Influenza: A Systematic Review and Meta-Analysis
Erratum in
-
Error in Size of Total Population.JAMA Intern Med. 2024 Jan 1;184(1):121. doi: 10.1001/jamainternmed.2023.4905. JAMA Intern Med. 2024. PMID: 37983038 Free PMC article. No abstract available.
-
Corrections to a Meta-Analysis of Oseltamivir Use in Preventing Hospitalization for Influenza.JAMA Intern Med. 2024 Jan 1;184(1):115-116. doi: 10.1001/jamainternmed.2023.4708. JAMA Intern Med. 2024. PMID: 37983045 No abstract available.
Abstract
Importance: Despite widespread use, summary evidence from prior meta-analyses has contradictory conclusions regarding whether oseltamivir decreases the risk of hospitalization when given to outpatients. Several large investigator-initiated randomized clinical trials have not yet been meta-analyzed.
Objective: To assess the efficacy and safety of oseltamivir in preventing hospitalization among influenza-infected adult and adolescent outpatients.
Data sources: PubMed, Ovid MEDLINE, Embase, Europe PubMed Central, Web of Science, Cochrane Central, ClinicalTrials.gov, and WHO International Clinical Trials Registry were searched from inception to January 4, 2022.
Study selection: Included studies were randomized clinical trials comparing oseltamivir vs placebo or nonactive controls in outpatients with confirmed influenza infection.
Data extraction and synthesis: In this systematic review and meta-analysis, Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines were followed. Two independent reviewers (R.H. and É.B.C.) extracted data and assessed risk of bias using the Cochrane Risk of Bias Tool 2.0. Each effect size was pooled using a restricted maximum likelihood random effects model. The quality of evidence was graded using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework.
Main outcomes and measures: Hospitalization was pooled as risk ratio (RR) and risk difference (RD) estimates with 95% CIs.
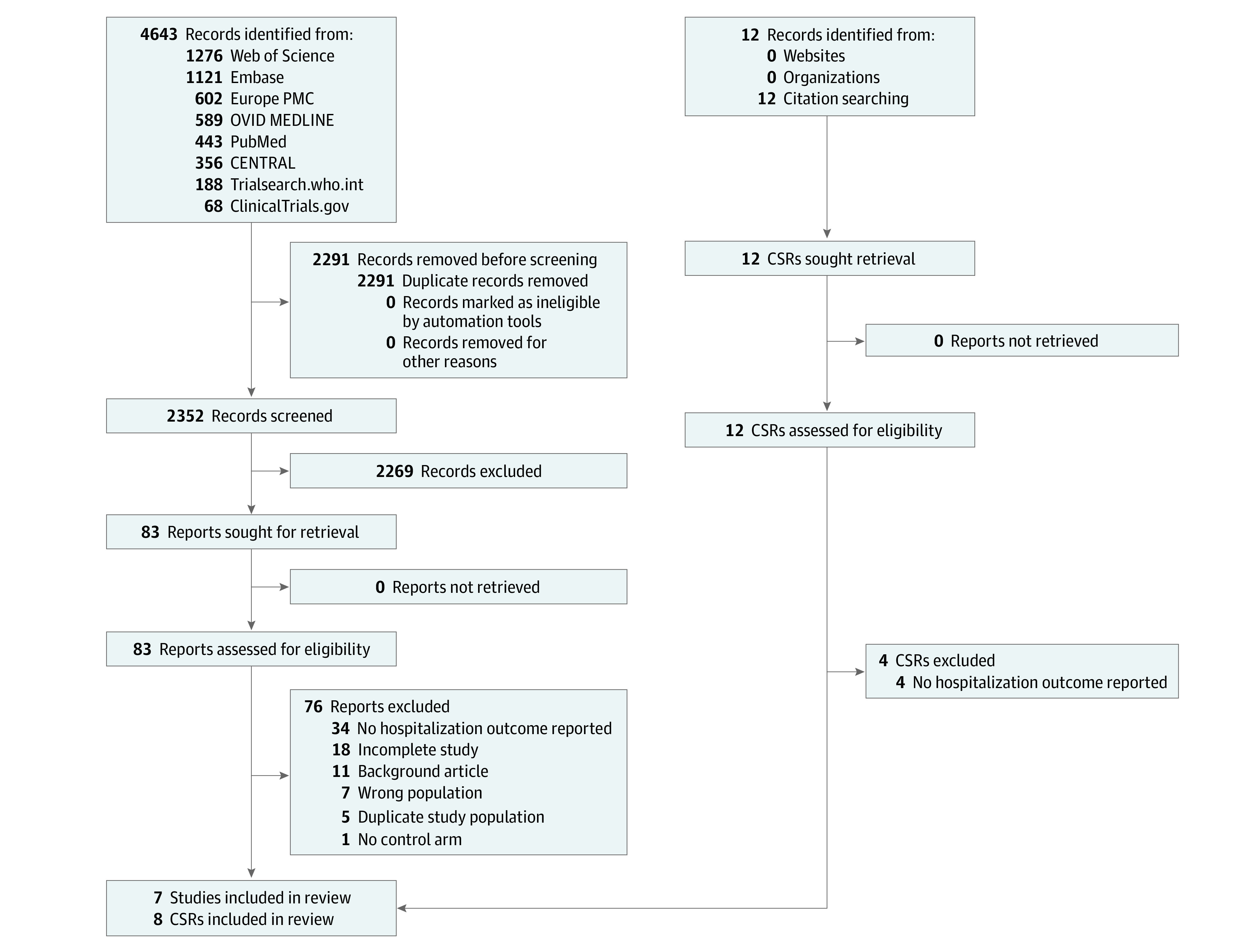
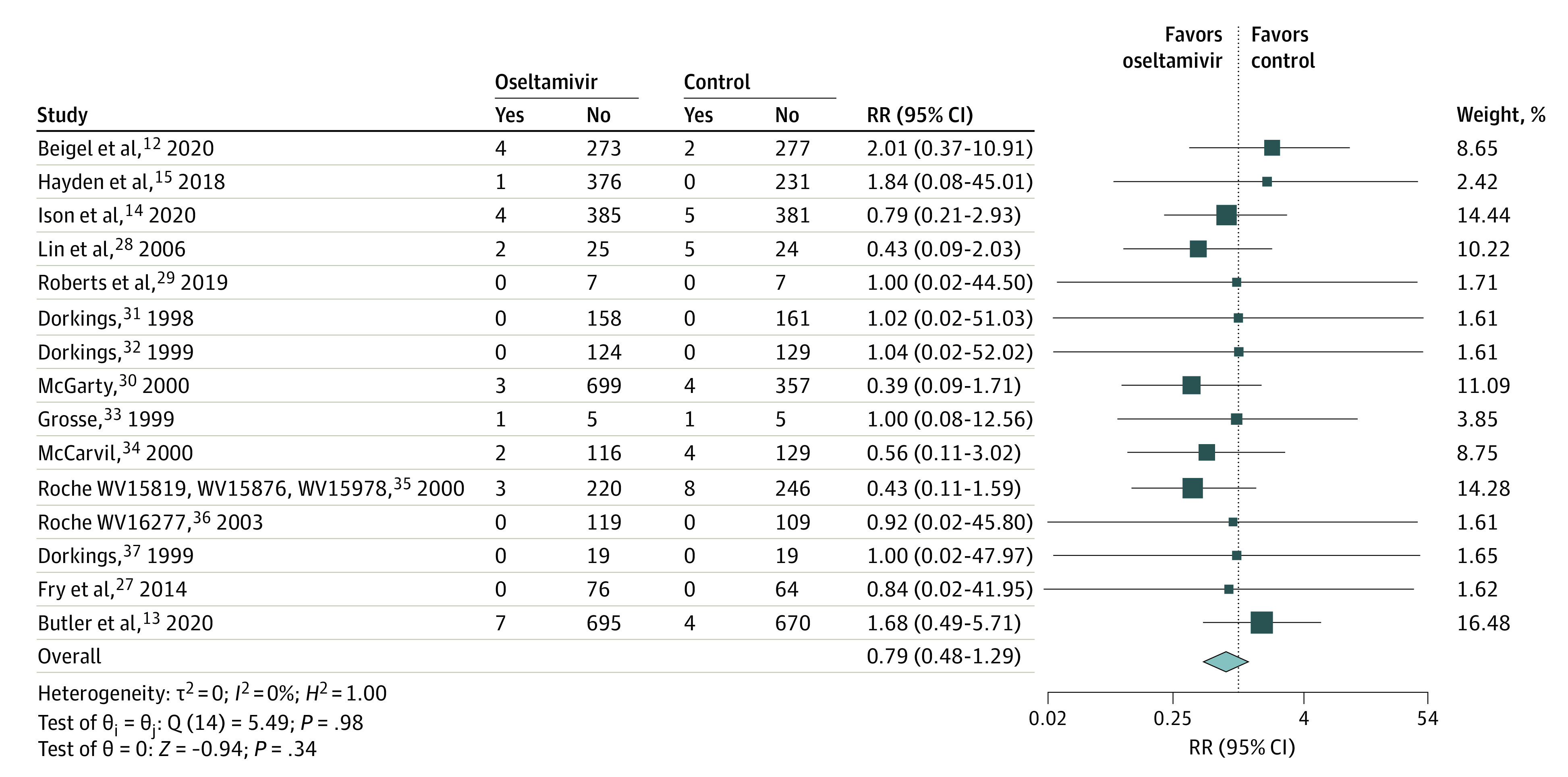
Results: Of 2352 studies identified, 15 were included. The intention-to-treat infected (ITTi) population was comprised of 6166 individuals with 54.7% prescribed oseltamivir. Across study populations, 53.9% (5610 of 10 471) were female and the mean age was 45.3 (14.5) years. Overall, oseltamivir was not associated with reduced risk of hospitalization within the ITTi population (RR, 0.79; 95% CI, 0.48 to 1.29; RD, -0.17%; 95% CI, -0.23% to 0.48%). Oseltamivir was also not associated with reduced hospitalization in older populations (mean age ≥65 years: RR, 1.01; 95% CI, 0.21 to 4.90) or in patients considered at greater risk of hospitalization (RR, 0.65; 0.33 to 1.28). Within the safety population, oseltamivir was associated with increased nausea (RR, 1.43; 95% CI, 1.13 to 1.82) and vomiting (RR, 1.83; 95% CI, 1.28 to 2.63) but not serious adverse events (RR, 0.71; 95% CI, 0.46 to1.08).
Conclusions and relevance: In this systematic review and meta-analysis among influenza-infected outpatients, oseltamivir was not associated with a reduced risk of hospitalization but was associated with increased gastrointestinal adverse events. To justify continued use for this purpose, an adequately powered trial in a suitably high-risk population is justified.
Conflict of interest statement
Figures
Comment in
-
Oseltamivir May or May Not Reduce Hospitalizations.JAMA Intern Med. 2024 Jan 1;184(1):116. doi: 10.1001/jamainternmed.2023.4711. JAMA Intern Med. 2024. PMID: 37983025 No abstract available.
-
Oseltamivir May or May Not Reduce Hospitalizations.JAMA Intern Med. 2024 Jan 1;184(1):116-117. doi: 10.1001/jamainternmed.2023.4720. JAMA Intern Med. 2024. PMID: 37983034 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention . Estimated flu-related illnesses, medical visits, hospitalizations, and deaths in the United States—2018–2019 flu season. 2020. Accessed May 2, 2023. https://www.cdc.gov/flu/about/burden/2018-2019.html
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
