

Epidemiology of Cancer-Associated Venous Thromboembolism in Patients With Solid and Hematologic Neoplasms in the Veterans Affairs Health Care System
- PMID: 37306999
- PMCID: PMC10261992
- DOI: 10.1001/jamanetworkopen.2023.17945
Epidemiology of Cancer-Associated Venous Thromboembolism in Patients With Solid and Hematologic Neoplasms in the Veterans Affairs Health Care System
Abstract
Importance: Identifying changes in epidemiologic patterns of the incidence and risk of cancer-associated thrombosis (CAT), particularly with evolving cancer-directed therapy, is essential for risk stratification.
Objective: To assess the incidence of CAT over time and to determine pertinent patient-specific, cancer-specific, and treatment-specific factors associated with its risk.
Design, setting, and participants: This longitudinal, retrospective cohort study was conducted from 2006 to 2021. Duration of follow-up was from the date of diagnosis until first venous thromboembolism (VTE) event, death, loss of follow-up (defined as a 90-day gap without clinical encounters), or administrative censoring on April 1, 2022. The study took place within the US Department of Veterans Affairs national health care system. Patients with newly diagnosed invasive solid tumors and hematologic neoplasms were included in the study. Data were analyzed from December 2022 to February 2023.
Exposure: Newly diagnosed invasive solid tumors and hematologic neoplasms.
Main outcomes: Incidence of VTE was assessed using a combination of International Classification of Diseases, Ninth Revision, Clinical Modification and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification and natural language processing confirmed outcomes. Cumulative incidence competing risk functions were used to estimate incidence of CAT. Multivariable Cox regression models were built to assess the association of baseline variables with CAT. Pertinent patient variables included demographics, region, rurality, area deprivation index, National Cancer Institute comorbidity index, cancer type, staging, first-line systemic treatment within 3 months (time-varying covariate), and other factors that could be associated with the risk of VTE.
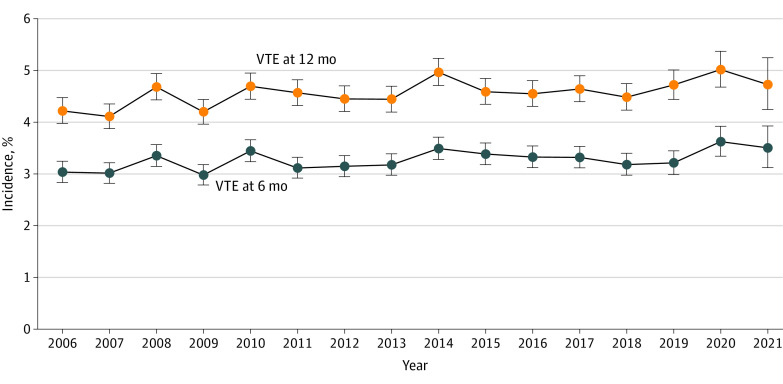
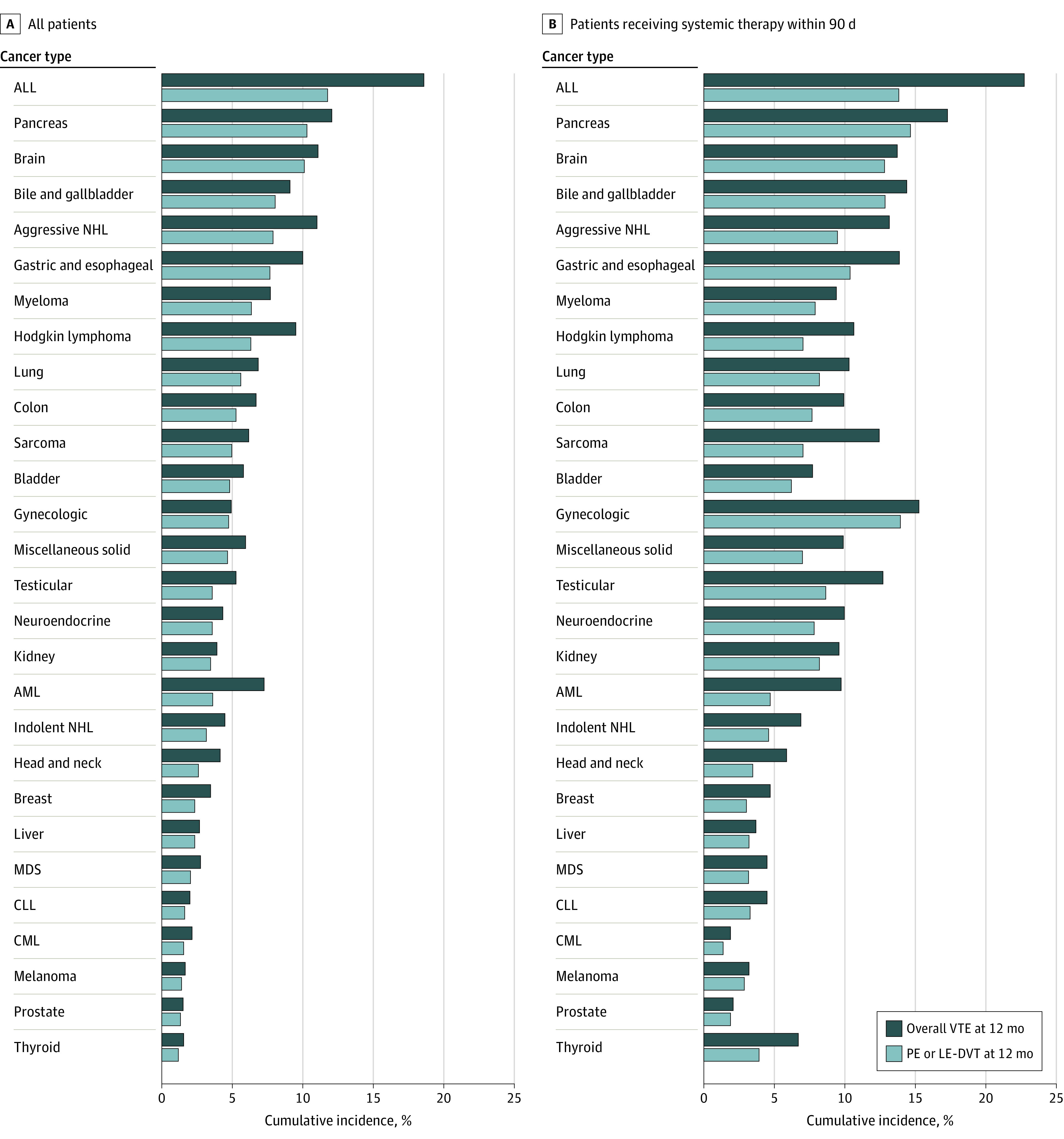
Results: A total of 434 203 patients (420 244 men [96.8%]; median [IQR] age, 67 [62-74] years; 7414 Asian or Pacific Islander patients [1.7%]; 20 193 Hispanic patients [4.7%]; 89 371 non-Hispanic Black patients [20.6%]; 313 157 non-Hispanic White patients [72.1%]) met the inclusion criteria. Overall incidence of CAT at 12 months was 4.5%, with yearly trends ranging stably from 4.2% to 4.7%. The risk of VTE was associated with cancer type and stage. In addition to confirming well-known risk distribution among patients with solid tumors, a higher risk of VTE was observed among patients with aggressive lymphoid neoplasms compared with patients with indolent lymphoid or myeloid hematologic neoplasms. Compared with no treatment, patients receiving first-line chemotherapy (hazard ratio [HR], 1.44; 95% CI, 1.40-1.49) and immune checkpoint inhibitors (HR, 1.49; 95% CI, 1.22-1.82) had a higher adjusted relative risk than patients receiving targeted therapy (HR, 1.21; 95% CI, 1.13-1.30) or endocrine therapy (HR, 1.20; 95% CI, 1.12-1.28). Finally, adjusted VTE risk was significantly higher among Non-Hispanic Black patients (HR, 1.23; 95% CI, 1.19-1.27) and significantly lower in Asian or Pacific Islander patients (HR, 0.84; 95% CI, 0.76-0.93) compared with Non-Hispanic White patients.
Conclusions and relevance: In this cohort study of patients with cancer, a high incidence of VTE was observed, with yearly trends that remained stable over the 16-year study period. Both novel and known factors associated with the risk of CAT were identified, providing valuable and applicable insights in this current treatment landscape.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
