

Poliprotect vs Omeprazole in the Relief of Heartburn, Epigastric Pain, and Burning in Patients Without Erosive Esophagitis and Gastroduodenal Lesions: A Randomized, Controlled Trial
- PMID: 37307528
- PMCID: PMC10617666
- DOI: 10.14309/ajg.0000000000002360
Poliprotect vs Omeprazole in the Relief of Heartburn, Epigastric Pain, and Burning in Patients Without Erosive Esophagitis and Gastroduodenal Lesions: A Randomized, Controlled Trial
Abstract
Introduction: In the treatment of upper GI endoscopy-negative patients with heartburn and epigastric pain or burning, antacids, antireflux agents, and mucosal protective agents are widely used, alone or as add-on treatment, to increase response to proton-pump inhibitors, which are not indicated in infancy and pregnancy and account for significant cost expenditure.
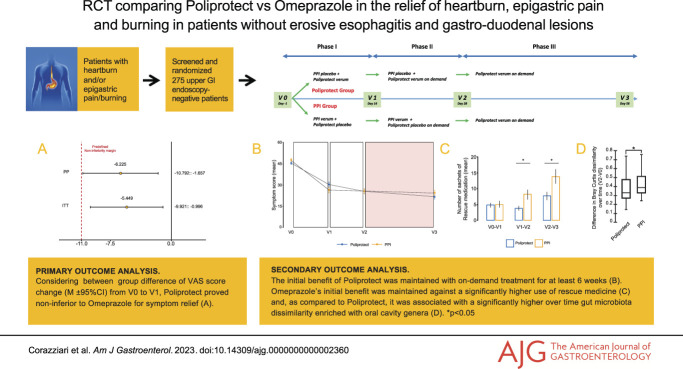
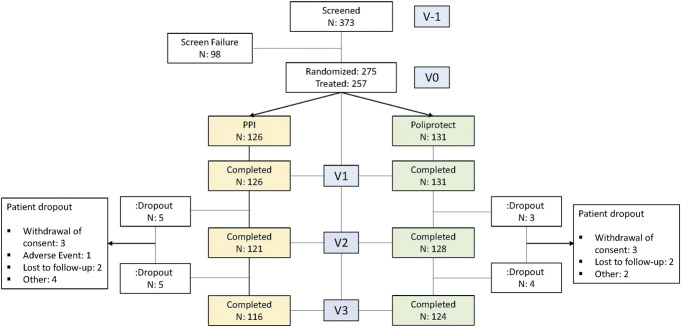
Methods: In this randomized, controlled, double-blind, double-dummy, multicenter trial assessing the efficacy and safety of mucosal protective agent Poliprotect (neoBianacid, Sansepolcro, Italy) vs omeprazole in the relief of heartburn and epigastric pain/burning, 275 endoscopy-negative outpatients were given a 4-week treatment with omeprazole (20 mg q.d.) or Poliprotect (5 times a day for the initial 2 weeks and on demand thereafter), followed by an open-label 4-week treatment period with Poliprotect on-demand. Gut microbiota change was assessed.
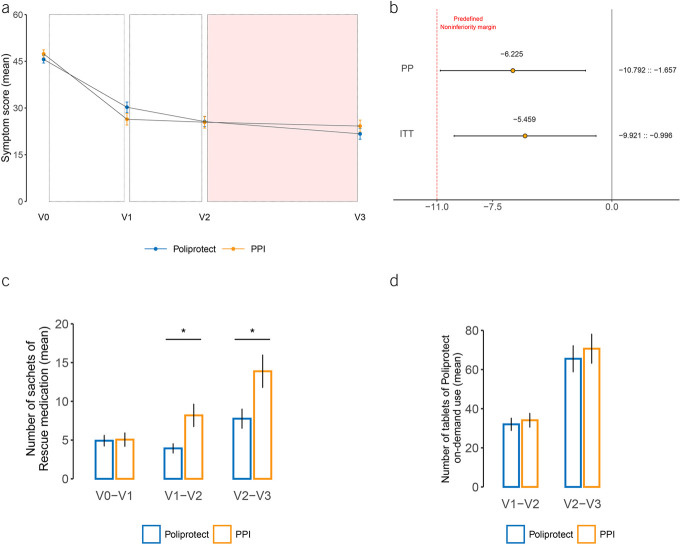
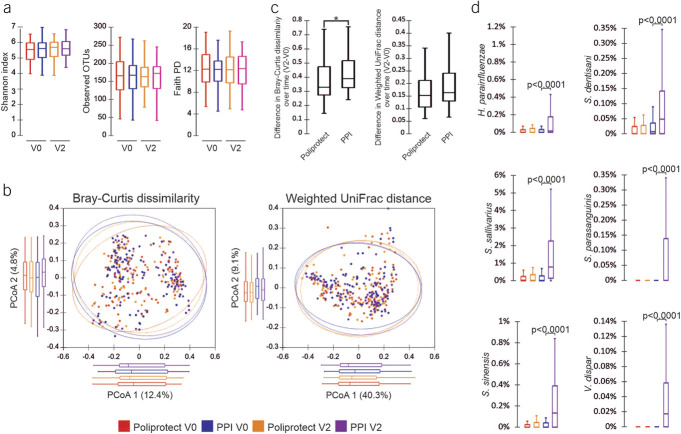
Results: A 2-week treatment with Poliprotect proved noninferior to omeprazole for symptom relief (between-group difference in the change in visual analog scale symptom score: [mean, 95% confidence interval] -5.4, -9.9 to -0.1; -6.2, -10.8 to -1.6; intention-to-treat and per-protocol populations, respectively). Poliprotect's benefit remained unaltered after shifting to on-demand intake, with no gut microbiota variation. The initial benefit of omeprazole was maintained against significantly higher use of rescue medicine sachets (mean, 95% confidence interval: Poliprotect 3.9, 2.8-5.0; omeprazole 8.2, 4.8-11.6) and associated with an increased abundance of oral cavity genera in the intestinal microbiota. No relevant adverse events were reported in either treatment arm.
Discussion: Poliprotect proved noninferior to standard-dose omeprazole in symptomatic patients with heartburn/epigastric burning without erosive esophagitis and gastroduodenal lesions. Gut microbiota was not affected by Poliprotect treatment. The study is registered in Clinicaltrial.gov (NCT03238534) and the EudraCT database (2015-005216-15).
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Sperber AD, Freud T, Aziz I, et al. Greater overlap of Rome IV disorders of gut-brain interactions leads to increased disease severity and poorer quality of life. Clin Gastroenterol Hepatol 2022;20:e945–e956. - PubMed
-
- Geeraerts A, Van Houtte B, Clevers E, et al. Gastroesophageal reflux disease-functional dyspepsia overlap: Do birds of a feather flock together? Am J Gastroenterol 2020;115:1167–82. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
