

doi: 10.1055/s-0043-1769936.
Epub 2023 Jun 12.
Current and Future Developments in Wound Healing
Affiliations
- PMID: 37308128
- PMCID: PMC11121504
- DOI: 10.1055/s-0043-1769936
Item in Clipboard
Current and Future Developments in Wound Healing
Facial Plast Surg.
2023 Oct.
Abstract
Poor wound healing on the face and neck can lead to significant morbidity and dissatisfaction in facial plastic surgery. With current advances in wound healing management and commercially available biologic and tissue-engineered products, there are several options available to optimize acute wound healing and treat delayed or chronic wounds. This article summarizes some of the key principals and recent developments in wound healing research in addition to potential future advancements in the field of soft tissue wound healing.
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures
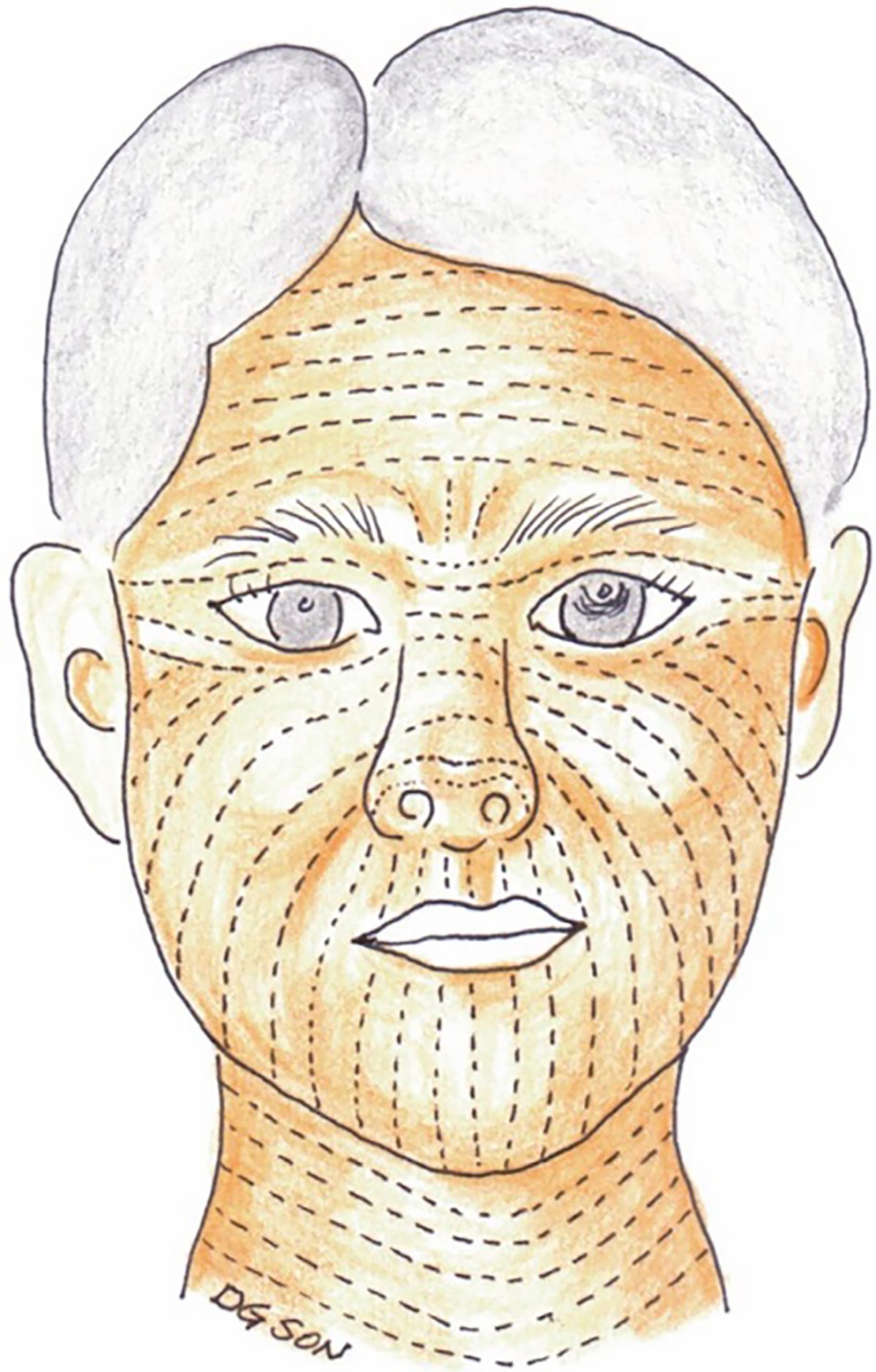
Relaxed skin tension lines (RSTLs) of the head and neck. These lines represent furrows created in the skin when the skin is pinched and relaxed without tension. Skin tension can be reduced when incisions are made parallel to RSTLs resulting in improved cosmesis and decreased risk of hypertrophic scarring. Langer’s lines (not shown) represent the direction of orientation of the underlying collagen fibers and run in the same direction as RSTLs in many areas of the body with the exception of the temple, lateral canthal area, and oral commissure. (Reprinted with permission from Son D, Harijan A. Overview of surgical scar prevention and management. J Korean Med Sci. 2014 Jun;29(6):751–7. doi: 10.3346/jkms.2014.29.6.751 . Epub 2014 May 30. PMID: 24932073; PMCID: PMC4055805.)
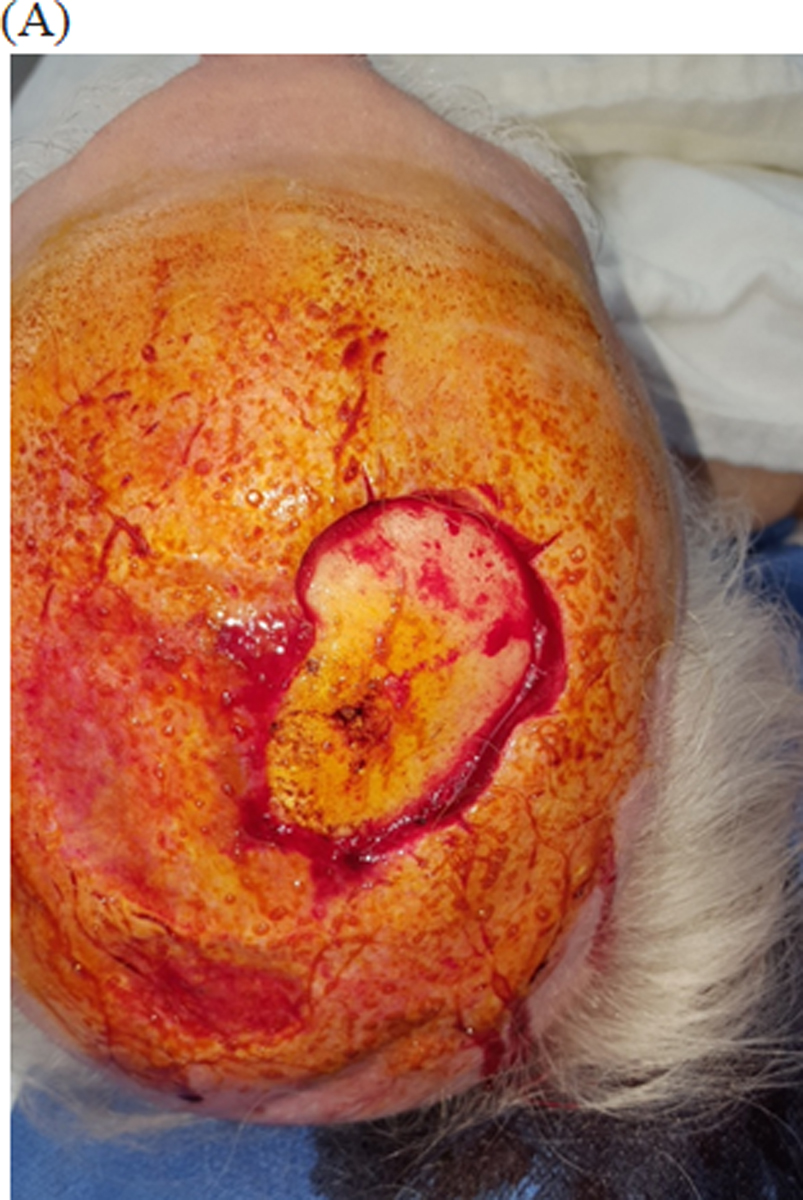
Integra bilayer used for reconstruction of scalp defect (A) 72 year male with bare calvarial bone defect after Mohs excision of basal cell carcinoma. (No periosteum present) (B) In a staged fashion Integra dressing was applied and secured for 1 month to induce granulation. (C) After 1 month, enough granulation tissue growth to receive a split thickness skin graft. (D) Two weeks after split thickness skin graft placement with good take of skin graft.

Integra bilayer used for reconstruction of scalp defect (A) 72 year male with bare calvarial bone defect after Mohs excision of basal cell carcinoma. (No periosteum present) (B) In a staged fashion Integra dressing was applied and secured for 1 month to induce granulation. (C) After 1 month, enough granulation tissue growth to receive a split thickness skin graft. (D) Two weeks after split thickness skin graft placement with good take of skin graft.

Integra bilayer used for reconstruction of scalp defect (A) 72 year male with bare calvarial bone defect after Mohs excision of basal cell carcinoma. (No periosteum present) (B) In a staged fashion Integra dressing was applied and secured for 1 month to induce granulation. (C) After 1 month, enough granulation tissue growth to receive a split thickness skin graft. (D) Two weeks after split thickness skin graft placement with good take of skin graft.

Integra bilayer used for reconstruction of scalp defect (A) 72 year male with bare calvarial bone defect after Mohs excision of basal cell carcinoma. (No periosteum present) (B) In a staged fashion Integra dressing was applied and secured for 1 month to induce granulation. (C) After 1 month, enough granulation tissue growth to receive a split thickness skin graft. (D) Two weeks after split thickness skin graft placement with good take of skin graft.
Similar articles
-
A contemporary review of wound healing in otolaryngology: current state and future promise.Laryngoscope. 2009 Nov;119(11):2099-110. doi: 10.1002/lary.20561. Laryngoscope. 2009. PMID: 19572395 Review.
-
New developments in wound healing relevant to facial plastic surgery.Arch Facial Plast Surg. 2008 Nov-Dec;10(6):402-6. doi: 10.1001/archfaci.10.6.402. Arch Facial Plast Surg. 2008. PMID: 19018061 Review.
-
Complex Wound Management.Facial Plast Surg. 2019 Dec;35(6):672-677. doi: 10.1055/s-0039-1700889. Epub 2019 Nov 29. Facial Plast Surg. 2019. PMID: 31783426
-
An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle.Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. Clin Orthop Relat Res. 2014. PMID: 24577615 Free PMC article.
-
Tissue Engineered Skin and Wound Healing: Current Strategies and Future Directions.Curr Pharm Des. 2017;23(24):3455-3482. doi: 10.2174/1381612823666170526094606. Curr Pharm Des. 2017. PMID: 28552069 Review.
