

Patiromer utility as an adjunct treatment in patients needing urgent hyperkalaemia management (PLATINUM): design of a multicentre, randomised, double-blind, placebo-controlled, parallel-group study
- PMID: 37308268
- PMCID: PMC10277034
- DOI: 10.1136/bmjopen-2022-071311
Patiromer utility as an adjunct treatment in patients needing urgent hyperkalaemia management (PLATINUM): design of a multicentre, randomised, double-blind, placebo-controlled, parallel-group study
Abstract
Introduction: Hyperkalaemia is common, life-threatening and often requires emergency department (ED) management; however, no standardised ED treatment protocol exists. Common treatments transiently reducing serum potassium (K+) (including albuterol, glucose and insulin) may cause hypoglycaemia. We outline the design and rationale of the Patiromer Utility as an Adjunct Treatment in Patients Needing Urgent Hyperkalaemia Management (PLATINUM) study, which will be the largest ED randomised controlled hyperkalaemia trial ever performed, enabling assessment of a standardised approach to hyperkalaemia management, as well as establishing a new evaluation parameter (net clinical benefit) for acute hyperkalaemia treatment investigations.
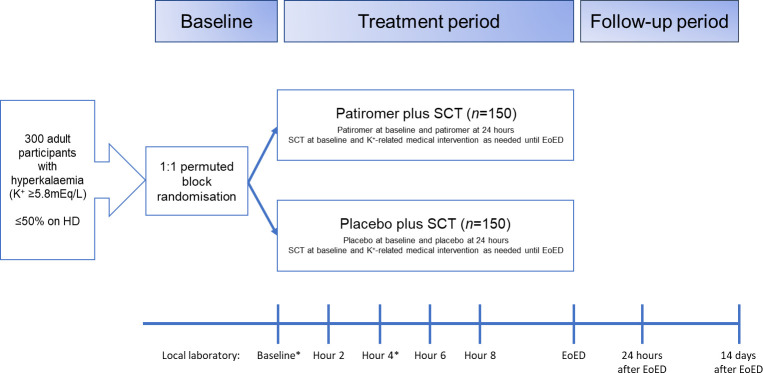
Methods and analysis: PLATINUM is a Phase 4, multicentre, randomised, double-blind, placebo-controlled study in participants who present to the ED at approximately 30 US sites. Approximately 300 adult participants with hyperkalaemia (K+ ≥5.8 mEq/L) will be enrolled. Participants will be randomised 1:1 to receive glucose (25 g intravenously <15 min before insulin), insulin (5 units intravenous bolus) and aerosolised albuterol (10 mg over 30 min), followed by a single oral dose of either 25.2 g patiromer or placebo, with a second dose of patiromer (8.4 g) or placebo after 24 hours. The primary endpoint is net clinical benefit, defined as the mean change in the number of additional interventions less the mean change in serum K+, at hour 6. Secondary endpoints are net clinical benefit at hour 4, proportion of participants without additional K+-related medical interventions, number of additional K+-related interventions and proportion of participants with sustained K+ reduction (K+ ≤5.5 mEq/L). Safety endpoints are the incidence of adverse events, and severity of changes in serum K+ and magnesium.
Ethics and dissemination: A central Institutional Review Board (IRB) and Ethics Committee provided protocol approval (#20201569), with subsequent approval by local IRBs at each site, and participants will provide written consent. Primary results will be published in peer-reviewed manuscripts promptly following study completion.
Trial registration number: NCT04443608.
Keywords: accident & emergency medicine; clinical trials; heart failure; hypertension.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ZR: Advisory board memberships (Cardiorenal disease) for AstraZeneca and CSL Vifor. JB: Employee and shareholder of CSL Vifor. CMQ: Employee and shareholder of CSL Vifor. YD: No relevant conflicts of interest to disclose. BS: NHLBI, CDC, Comprehensive Research Associates (institutional grants). JJB: No relevant conflicts of interest to disclose. BED: No relevant conflicts of interest to disclose. CAH: Personal fees (consultant) from AstraZeneca, Bayer, Diamedica, FibroGen, Merck, NxStage, Pfizer, Relypsa, University of Oxford, Bristol Myers Squibb; Grants from the University of British Columbia and Bristol Myers Squibb and the National Institutes of Health (NIDDK and NHLBI), and author royalties from UpToDate. Stock ownership in Johnson & Johnson, Merck, and Pfizer. Employee of Hennepin Healthcare. MRW: Consulting fees: CSL Vifor and AstraZeneca. Honoraria: CSL Vifor. AJS: Research grants: Comprehensive Research Associates. Consulting fees: AstraZeneca. SB: No relevant conflicts of interest to disclose. KMS-R: No relevant conflicts of interest to disclose. WFP: Research Grants: Brainbox, Instrument Labs, Salix. Consultant: Abbott, Brainbox, Instrument Labs, Janssen, Osler, Roche, Siemens, CSL Vifor. Stock/Ownership Interests: AseptiScope Inc, Brainbox Inc, Braincheck Inc, Coagulo Inc, Comprehensive Research Associates LLC, Comprehensive Research Management Inc, Emergencies in Medicine LLC, Fast Inc, Forrest Devices, Ischemia DX LLC, Lucia Inc, Prevencio Inc, RCE Technologies, ROMTech, ScPharma, Trivirum Inc, Upstream Inc.
Figures

References
-
- Quality AfHRa . Healthcare cost and utilization project (Hcupnet). n.d. Available: https://datatools.ahrq.gov/hcupnet
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical