

Prenatal opioid exposure and well-child care in the first 2 years of life: population-based cohort study
- PMID: 37308290
- PMCID: PMC10447387
- DOI: 10.1136/archdischild-2022-325029
Prenatal opioid exposure and well-child care in the first 2 years of life: population-based cohort study
Abstract
Objectives: To quantify well-child visits by age 2 years and developmental screening at the 18-month enhanced well-child visit among children with prenatal opioid exposure (POE) and to identify factors associated with study outcomes.
Design: Population-based cohort study.
Setting: Ontario, Canada.
Participants: 22 276 children with POE born 2014-2018 were classified as (1) 1-29 days of prescribed opioid analgesia, (2) 30+ days of prescribed opioid analgesia, (3) medication for opioid use disorder (MOUD), (4) MOUD and opioid analgesia, or (5) unregulated opioids.
Main outcome measures: Attending ≥5 well-child visits by age 2 years and the 18-month enhanced well-child visit. Modified Poisson regression was used to examine factors associated with outcomes.
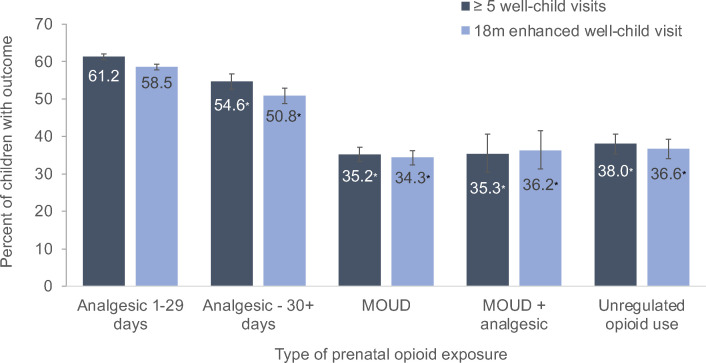
Results: Children with POE to 1-29 days of analgesics were most likely to attend ≥5 well-child visits (61.2%). Compared with these children, adjusted relative risks (aRRs) for ≥5 well-child visits were lower among those exposed to 30+ days of opioid analgesics (0.95, 95% CI 0.91 to 0.99), MOUD (0.83, 95% CI 0.79 to 0.88), MOUD and opioid analgesics (0.78 95% CI 0.68 to 0.90) and unregulated opioids (0.89, 95% CI 0.83 to 0.95). Relative to children with POE to 1-29 days of analgesics (58.5%), respective aRRs for the 18-month enhanced well-child visit were 0.92 (95% CI 0.88 to 0.96), 0.76 (95% CI 0.72 to 0.81), 0.76 (95% CI 0.66 to 0.87) and 0.82 (95% CI 0.76 to 0.88). Having a regular primary care provider was positively associated with study outcomes; socioeconomic disadvantage, rurality and maternal mental health were negatively associated.
Conclusion: Well-child visits are low in children following POE, especially among offspring of mothers receiving MOUD or unregulated opioids. Strategies to improve attendance will be important for child outcomes.
Keywords: Child Development; Epidemiology; Healthcare Disparities; Paediatrics; Primary Health Care.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Prenatal Opioid Exposure and Immune-Related Conditions in Children.JAMA Netw Open. 2024 Jan 2;7(1):e2351933. doi: 10.1001/jamanetworkopen.2023.51933. JAMA Netw Open. 2024. PMID: 38231512 Free PMC article.
-
Health outcomes in children with prenatal opioid exposure with and without neonatal abstinence syndrome in the first seven years of life: An observational cohort study.J Nurs Scholarsh. 2024 Nov;56(6):767-779. doi: 10.1111/jnu.13000. Epub 2024 Jun 21. J Nurs Scholarsh. 2024. PMID: 39560001
-
Impact of maternal medication for opioid use disorder on neurodevelopmental outcomes of infants treated for neonatal opioid withdrawal syndrome.J Neonatal Perinatal Med. 2021;14(4):463-473. doi: 10.3233/NPM-200615. J Neonatal Perinatal Med. 2021. PMID: 33843701
-
Cognitive and Motor Outcomes of Children With Prenatal Opioid Exposure: A Systematic Review and Meta-analysis.JAMA Netw Open. 2019 Jul 3;2(7):e197025. doi: 10.1001/jamanetworkopen.2019.7025. JAMA Netw Open. 2019. PMID: 31298718 Free PMC article.
-
Effects of prenatal opioid exposure on synaptic adaptations and behaviors across development.Neuropharmacology. 2023 Jan 1;222:109312. doi: 10.1016/j.neuropharm.2022.109312. Epub 2022 Nov 2. Neuropharmacology. 2023. PMID: 36334764 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical