

The network structure of mania symptoms differs between people with and without binge eating
- PMID: 37308319
- PMCID: PMC10768381
- DOI: 10.1111/bdi.13355
The network structure of mania symptoms differs between people with and without binge eating
Abstract
Objectives: People with bipolar disorder who also report binge eating have increased psychopathology and greater impairment than those without binge eating. Whether this co-occurrence is related to binge eating as a symptom or presents differently across full-syndrome eating disorders with binge eating is unclear.
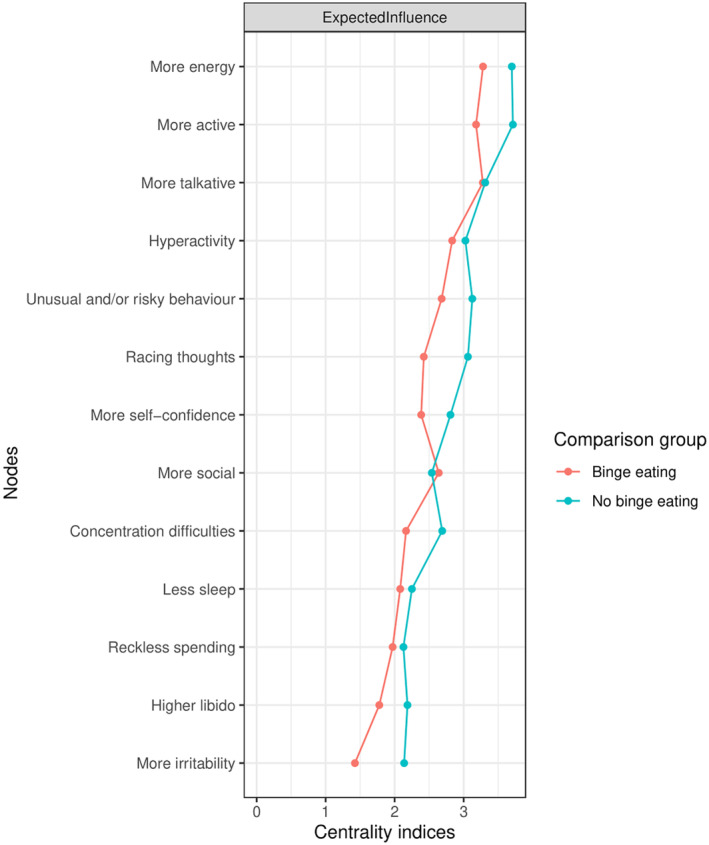
Methods: We first compared networks of 13 lifetime mania symptoms in 34,226 participants from the United Kingdom's National Institute for Health and Care Research BioResource with (n = 12,104) and without (n = 22,122) lifetime binge eating. Second, in the subsample with binge eating, we compared networks of mania symptoms in participants with lifetime anorexia nervosa binge-eating/purging (n = 825), bulimia nervosa (n = 3737), and binge-eating disorder (n = 3648).
Results: People with binge eating endorsed every mania symptom significantly more often than those without binge eating. Within the subsample, people with bulimia nervosa most often had the highest endorsement rate of each mania symptom. We found significant differences in network parameter statistics, including network structure (M = 0.25, p = 0.001) and global strength (S = 1.84, p = 0.002) when comparing the binge eating with no binge-eating participants. However, network structure differences were sensitive to reductions in sample size and the greater density of the latter network was explained by the large proportion of participants (34%) without mania symptoms. The structure of the anorexia nervosa binge-eating/purging network differed from the bulimia nervosa network (M = 0.66, p = 0.001), but the result was unstable.
Conclusions: Our results suggest that the presence and structure of mania symptoms may be more associated with binge eating as a symptom rather than any specific binge-type eating disorder. Further research with larger sample sizes is required to confirm our findings.
Keywords: anorexia nervosa; binge-eating disorder; bipolar disorder; bulimia nervosa; diagnosis; network analysis; signs and symptoms.
© 2023 The Authors. Bipolar Disorders published by John Wiley & Sons Ltd.
Conflict of interest statement
Prof Breen has received honoraria, research or conference grants and consulting fees from Illumina, Otsuka, and COMPASS Pathfinder Ltd. Prof Walters has received grant funding from Takeda for work unrelated to the GLAD Study. The remaining authors have nothing to disclose.
Figures





References
-
- Thiebaut S, Godart N, Radon L, Courtet P, Guillaume S. Crossed prevalence results between subtypes of eating disorder and bipolar disorder: a systematic review of the literature. Encephale. 2019;45:60‐73. - PubMed
-
- McElroy SL, Kotwal R, Keck PE Jr. Comorbidity of eating disorders with bipolar disorder and treatment implications. Bipolar Disord. 2006;8:686‐695. - PubMed
-
- McElroy SL, Crow S, Blom TJ, et al. Clinical features of bipolar spectrum with binge eating behaviour. J Affect Disord. 2016;201:95‐98. - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders (DSM‐5®). American Psychiatric Pub; 2013.
-
- Tseng M‐CM, Chang C‐H, Chen K‐Y, Liao S‐C, Chen H‐C. Prevalence and correlates of bipolar disorders in patients with eating disorders. J Affect Disord. 2016;190:599‐606. - PubMed
