

Interplay of hypoxia-inducible factors and oxygen therapy in cardiovascular medicine
- PMID: 37308571
- PMCID: PMC11014460
- DOI: 10.1038/s41569-023-00886-y
Interplay of hypoxia-inducible factors and oxygen therapy in cardiovascular medicine
Abstract
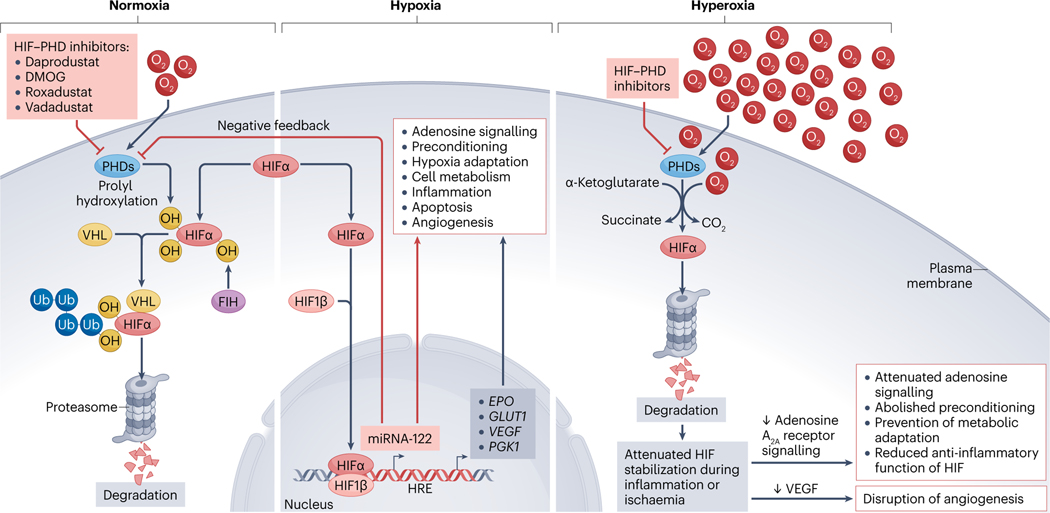
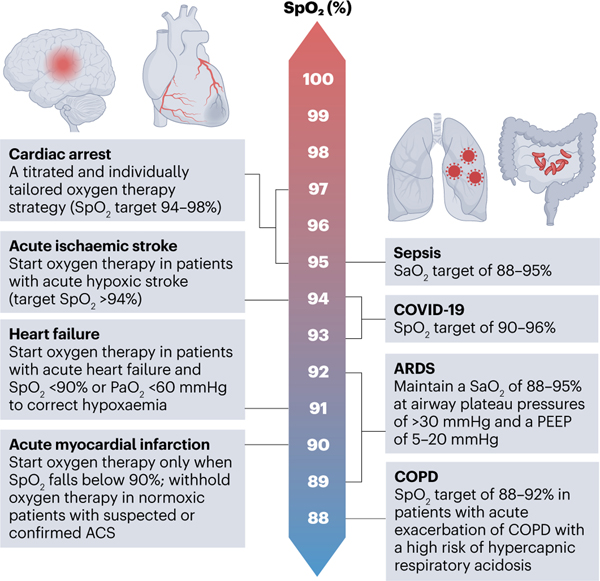
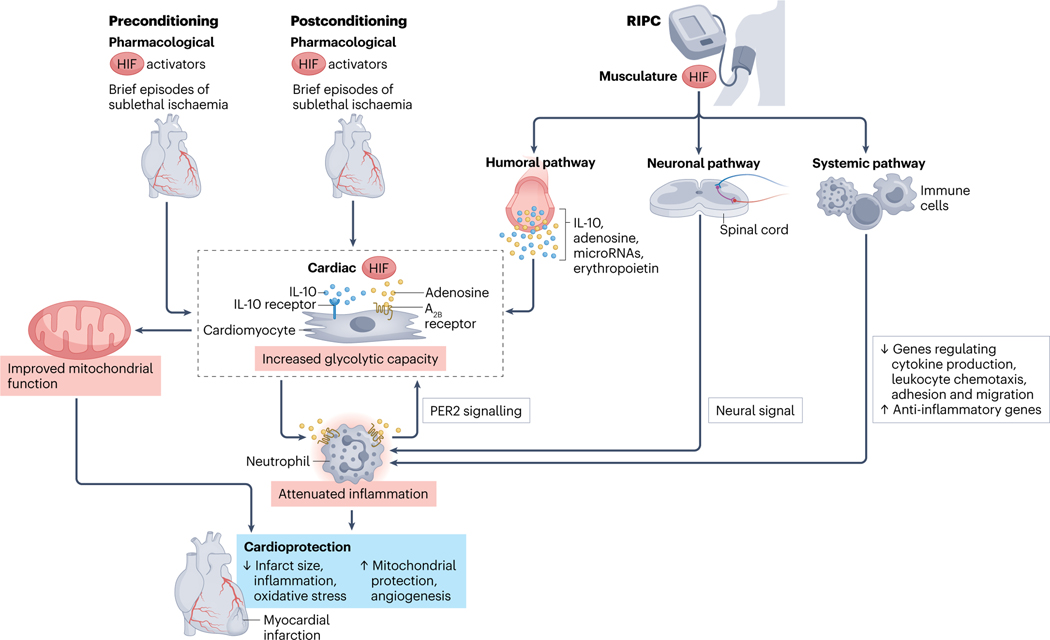
Mammals have evolved to adapt to differences in oxygen availability. Although systemic oxygen homeostasis relies on respiratory and circulatory responses, cellular adaptation to hypoxia involves the transcription factor hypoxia-inducible factor (HIF). Given that many cardiovascular diseases involve some degree of systemic or local tissue hypoxia, oxygen therapy has been used liberally over many decades for the treatment of cardiovascular disorders. However, preclinical research has revealed the detrimental effects of excessive use of oxygen therapy, including the generation of toxic oxygen radicals or attenuation of endogenous protection by HIFs. In addition, investigators in clinical trials conducted in the past decade have questioned the excessive use of oxygen therapy and have identified specific cardiovascular diseases in which a more conservative approach to oxygen therapy could be beneficial compared with a more liberal approach. In this Review, we provide numerous perspectives on systemic and molecular oxygen homeostasis and the pathophysiological consequences of excessive oxygen use. In addition, we provide an overview of findings from clinical studies on oxygen therapy for myocardial ischaemia, cardiac arrest, heart failure and cardiac surgery. These clinical studies have prompted a shift from liberal oxygen supplementation to a more conservative and vigilant approach to oxygen therapy. Furthermore, we discuss the alternative therapeutic strategies that target oxygen-sensing pathways, including various preconditioning approaches and pharmacological HIF activators, that can be used regardless of the level of oxygen therapy that a patient is already receiving.
© 2023. Springer Nature Limited.
Figures

Similar articles
-
Keeping the engine primed: HIF factors as key regulators of cardiac metabolism and angiogenesis during ischemia.J Mol Med (Berl). 2007 Dec;85(12):1309-15. doi: 10.1007/s00109-007-0279-x. Epub 2007 Nov 20. J Mol Med (Berl). 2007. PMID: 18026917 Review.
-
Adaptive and maladaptive cardiorespiratory responses to continuous and intermittent hypoxia mediated by hypoxia-inducible factors 1 and 2.Physiol Rev. 2012 Jul;92(3):967-1003. doi: 10.1152/physrev.00030.2011. Physiol Rev. 2012. PMID: 22811423 Free PMC article. Review.
-
miRNAs regulate the HIF switch during hypoxia: a novel therapeutic target.Angiogenesis. 2018 May;21(2):183-202. doi: 10.1007/s10456-018-9600-2. Epub 2018 Jan 27. Angiogenesis. 2018. PMID: 29383635 Free PMC article. Review.
-
The medical use of oxygen: a time for critical reappraisal.J Intern Med. 2013 Dec;274(6):505-28. doi: 10.1111/joim.12139. J Intern Med. 2013. PMID: 24206183 Review.
-
Genetic approaches to understand cellular responses to oxygen availability.FEBS J. 2022 Sep;289(18):5396-5412. doi: 10.1111/febs.16072. Epub 2021 Jun 26. FEBS J. 2022. PMID: 34125486 Review.
Cited by
-
The BMAL1/HIF2A heterodimer modulates circadian variations of myocardial injury.Res Sq [Preprint]. 2024 Feb 28:rs.3.rs-3938716. doi: 10.21203/rs.3.rs-3938716/v1. Res Sq. 2024. Update in: Nature. 2025 May;641(8064):1017-1028. doi: 10.1038/s41586-025-08898-z. PMID: 38464103 Free PMC article. Updated. Preprint.
-
Living Therapeutics for Synergistic Hydrogen-Photothermal Cancer Treatment by Photosynthetic Bacteria.Adv Sci (Weinh). 2025 Jan;12(1):e2408807. doi: 10.1002/advs.202408807. Epub 2024 Nov 4. Adv Sci (Weinh). 2025. PMID: 39495651 Free PMC article.
-
Spatial adjustment of bioenergetics, a possible determinant of contractile adaptation and development of contractile failure.Front Mol Med. 2023 Dec 6;3:1305960. doi: 10.3389/fmmed.2023.1305960. eCollection 2023. Front Mol Med. 2023. PMID: 39086691 Free PMC article. Review.
-
The context-dependent epigenetic and organogenesis programs determine 3D vs. 2D cellular fitness of MYC-driven murine liver cancer cells.Res Sq [Preprint]. 2025 Jan 7:rs.3.rs-4390765. doi: 10.21203/rs.3.rs-4390765/v4. Res Sq. 2025. Update in: Elife. 2025 May 06;14:RP101299. doi: 10.7554/eLife.101299. PMID: 38853928 Free PMC article. Updated. Preprint.
-
Progressive Deactivation of Hydroxylases Controls Hypoxia-Inducible Factor-1α-Coordinated Cellular Adaptation to Graded Hypoxia.Research (Wash D C). 2025 Apr 1;8:0651. doi: 10.34133/research.0651. eCollection 2025. Research (Wash D C). 2025. PMID: 40171017 Free PMC article.
References
-
- Steele C. Severe angina pectoris relieved by oxygen inhalations.Br. Med. J. 2, 1568 (1900).
-
- Heffner JE The story of oxygen. Respir. Care 58, 18–31 (2013). - PubMed
-
- Shultz SM & Hartmann PM George E Holtzapple (1862–1946) and oxygen therapy for lobar pneumonia: the first reported case (1887) and a review of the contemporary literature to 1899. J. Med. Biogr. 13, 201–206 (2005). - PubMed
-
- Severinghaus JW Eight sages over five centuries share oxygen’s discovery. Adv. Physiol. Educ. 40, 370–376 (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
