

Risk factors for disease severity among children with Covid-19: a clinical prediction model
- PMID: 37308825
- PMCID: PMC10259359
- DOI: 10.1186/s12879-023-08357-y
Risk factors for disease severity among children with Covid-19: a clinical prediction model
Abstract
Background: Children account for a significant proportion of COVID-19 hospitalizations, but data on the predictors of disease severity in children are limited. We aimed to identify risk factors associated with moderate/severe COVID-19 and develop a nomogram for predicting children with moderate/severe COVID-19.
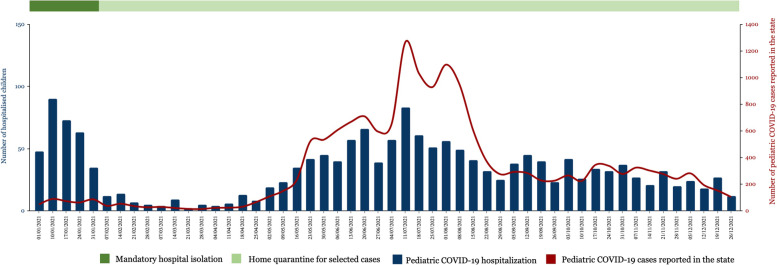
Methods: We identified children ≤ 12 years old hospitalized for COVID-19 across five hospitals in Negeri Sembilan, Malaysia, from 1 January 2021 to 31 December 2021 from the state's pediatric COVID-19 case registration system. The primary outcome was the development of moderate/severe COVID-19 during hospitalization. Multivariate logistic regression was performed to identify independent risk factors for moderate/severe COVID-19. A nomogram was constructed to predict moderate/severe disease. The model performance was evaluated using the area under the curve (AUC), sensitivity, specificity, and accuracy.
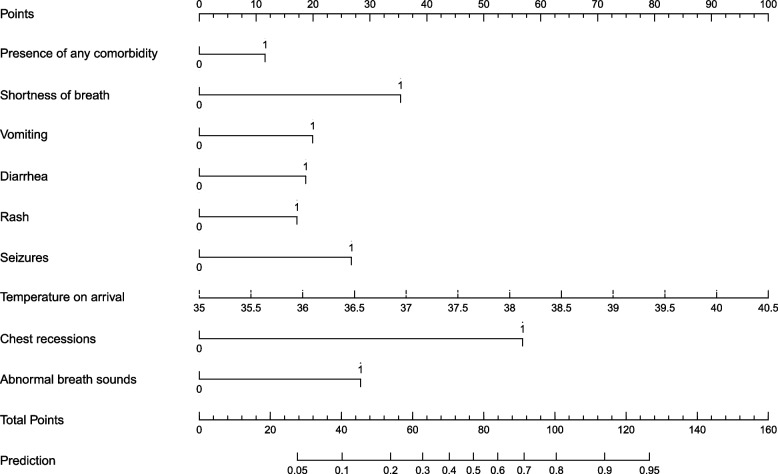
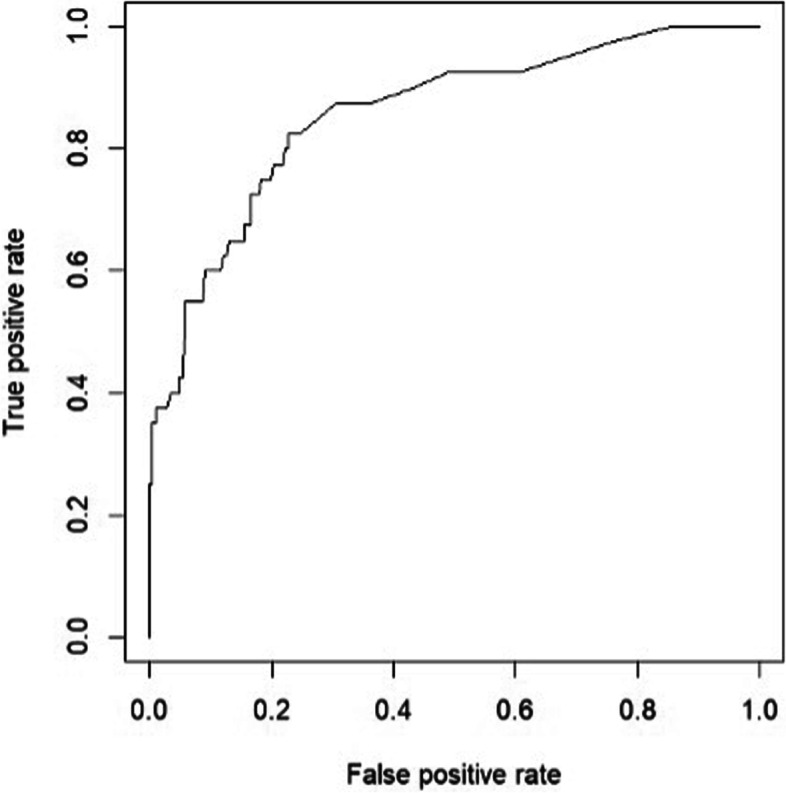
Results: A total of 1,717 patients were included. After excluding the asymptomatic cases, 1,234 patients (1,023 mild cases and 211 moderate/severe cases) were used to develop the prediction model. Nine independent risk factors were identified, including the presence of at least one comorbidity, shortness of breath, vomiting, diarrhea, rash, seizures, temperature on arrival, chest recessions, and abnormal breath sounds. The nomogram's sensitivity, specificity, accuracy, and AUC for predicting moderate/severe COVID-19 were 58·1%, 80·5%, 76·8%, and 0·86 (95% CI, 0·79 - 0·92) respectively.
Conclusion: Our nomogram, which incorporated readily available clinical parameters, would be useful to facilitate individualized clinical decisions.
Keywords: COVID-19; Nomogram; Pediatric; Predictor severity.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
