

XENERA-1: a randomised double-blind Phase II trial of xentuzumab in combination with everolimus and exemestane versus everolimus and exemestane in patients with hormone receptor-positive/HER2-negative metastatic breast cancer and non-visceral disease
- PMID: 37308971
- PMCID: PMC10258741
- DOI: 10.1186/s13058-023-01649-w
XENERA-1: a randomised double-blind Phase II trial of xentuzumab in combination with everolimus and exemestane versus everolimus and exemestane in patients with hormone receptor-positive/HER2-negative metastatic breast cancer and non-visceral disease
Abstract
Background: Xentuzumab is a humanised monoclonal antibody that binds to IGF-1 and IGF-2, neutralising their proliferative activity and restoring inhibition of AKT by everolimus. This study evaluated the addition of xentuzumab to everolimus and exemestane in patients with advanced breast cancer with non-visceral disease.
Methods: This double-blind, randomised, Phase II study was undertaken in female patients with hormone-receptor (HR)-positive/human epidermal growth factor 2 (HER2)-negative advanced breast cancer with non-visceral disease who had received prior endocrine therapy with or without CDK4/6 inhibitors. Patients received a weekly intravenous infusion of xentuzumab (1000 mg) or placebo in combination with everolimus (10 mg/day orally) and exemestane (25 mg/day orally). The primary endpoint was progression-free survival (PFS) per independent review.
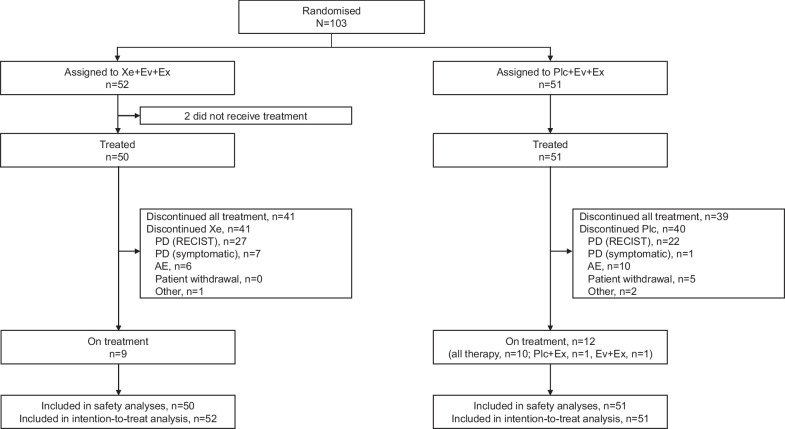
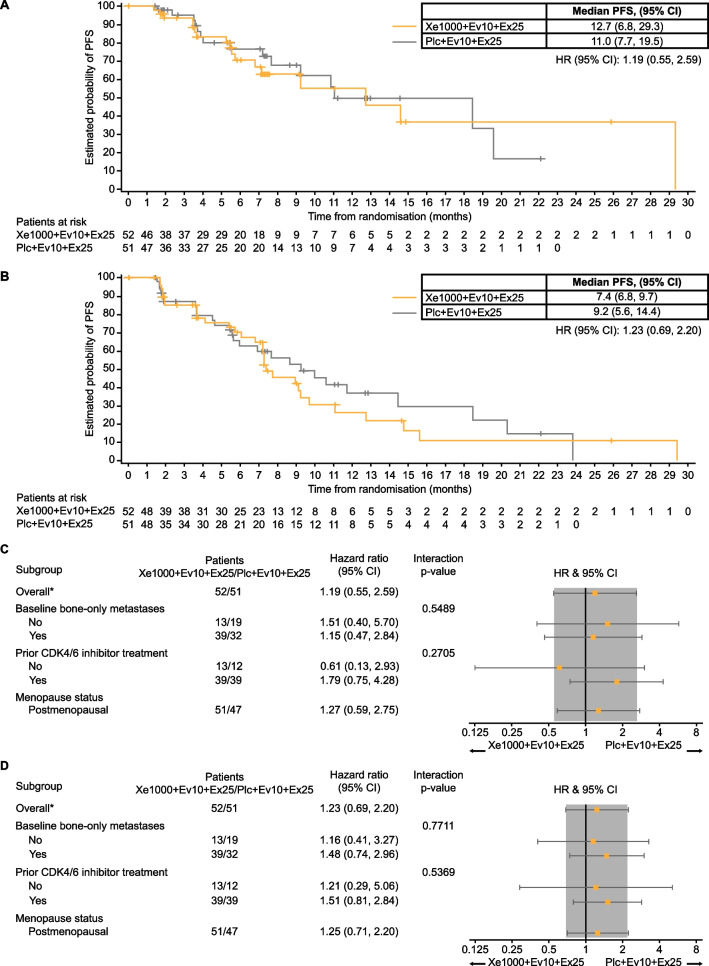
Results: A total of 103 patients were randomised and 101 were treated (n = 50 in the xentuzumab arm and n = 51 in the placebo arm). The trial was unblinded early due to high rates of discordance between independent and investigator assessment of PFS. Per independent assessment, median PFS was 12.7 (95% CI 6.8-29.3) months with xentuzumab and 11.0 (7.7-19.5) months with placebo (hazard ratio 1.19; 95% CI 0.55-2.59; p = 0.6534). Per investigator assessment, median PFS was 7.4 (6.8-9.7) months with xentuzumab and 9.2 (5.6-14.4) months with placebo (hazard ratio 1.23; 95% CI 0.69-2.20; p = 0.4800). Tolerability was similar between the arms, with diarrhoea (33.3-56.0%), fatigue (33.3-44.0%) and headache (21.6-40.0%) being the most common treatment-emergent adverse events. The incidence of grade ≥ 3 hyperglycaemia was similar between the xentuzumab (2.0%) and placebo (5.9%) arms.
Conclusions: While this study demonstrated that xentuzumab could be safely combined with everolimus and exemestane in patients with HR-positive/HER2-negative advanced breast cancer with non-visceral disease, there was no PFS benefit with the addition of xentuzumab. Trial registration ClinicalTrials.gov, NCT03659136. Prospectively registered, September 6, 2018.
Keywords: Advanced breast cancer; Everolimus; Exemestane; HR+/HER2−; Insulin-like growth factor; Non-visceral disease; Xentuzumab.
© 2023. The Author(s).
Conflict of interest statement
Peter Schmid reports receiving consultancy fees/honorarium from AstraZeneca, Bayer, Boehringer Ingelheim, Merck, Novartis, Pfizer, Puma, Roche, Eisai, and Celgene; receiving institutional funding from Astellas, AstraZeneca, Genentech, Novartis, OncoGenex, Roche, and Medivation; and having an immediate family member employed by Roche. Javier Cortes reports receiving fees for consulting/advisor roles with Roche, Celgene, Cellestia, AstraZeneca, Seattle Genetics, Daiichi Sankyo, Erytech, Athenex, Polyphor, Lilly, Merck Sharp & Dohme, GSK, Leuko, Bioasis, Clovis Oncology, Boehringer Ingelheim, Ellipses, Hibercell, BioInvent, Gemoab, Gilead, Menarini, Zymeworks, Reveal Genomics; receiving honoraria from Roche, Novartis, Celgene, Eisai, Pfizer, Samsung Bioepis, Lilly, Merck Sharp & Dohme, Daiichi Sankyo; holding stock, patents and intellectual property with MedSIR, Nektar Pharmaceuticals; and travel, accommodation, expenses from Roche, Novartis, Eisai, Pfizer, Daiichi Sankyo, AstraZeneca. Ana Joaquim has received fees for consulting/advisor roles, in the last 3 years, from Daiichi Sankyo, Eisai, Gilead, Glaxo Smith Kline, Lilly, Merck, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Vifor Pharma and Zuellig Pharma. Julie Lemieux has served in a consultancy or advisory role and received honorarium from Novartis, Eli Lilly, Gilead, Pfizer, and AstraZeneca; and has received research funding from Celgene, Genentech, GlaxoSmithKline, Roche, Millennium, Novartis, Merck Gilead, Abbvie, Acerta, Bayer, Pfizer, BMS, Esai, Sanofi, Janssen, Ozmosys, Sierra AstraZeneca, and Takeda. José Ángel García-Sáenz reported grants from SeaGen, Gilead, Eli Lilly and Company, AstraZeneca, and Daiichi Sankyo; and personal fees from Novartis, Eisai, and Merck Sharp & Dohme. Lowell Hart serves on the advisory boards and consults for Novartis, G1 Therapeutics, Seattle Genetics, AstraZeneca, and Nanostring. Tsvetan Biyukov, Navid Baktash are employees of Boehringer Ingelheim. Dan Massey is an employee of Elderbrook Solutions contracted by Boehringer Ingelheim. Hope Rugo reports receiving honoraria from Puma Biotechnology, Mylan, Samsung Bioepis, Chugai Pharma, Blueprint Medicines; receiving fees for a consulting or advisory role with Napo Pharmaceuticals; and institutional research funding from OBI Pharma, Pfizer, Novartis, Lilly, Genentech, Merck, Odonate Therapeutics, Daiichi Sankyo, Sermonix Pharmaceuticals, AstraZeneca, Gilead Sciences, Ayala Pharmaceuticals, Astellas Pharma, Seattle Genetics, MacroGenics, Boehringer Ingelheim, Polyphor. All other authors report no conflicts of interest.
Figures
References
-
- Gennari A, Andre F, Barrios CH, Cortes J, de Azambuja E, DeMichele A, Dent R, Fenlon D, Gligorov J, Hurvitz SA, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. doi: 10.1016/j.annonc.2021.09.019. - DOI - PubMed
-
- Rozenblit M, Mun S, Soulos P, Adelson K, Pusztai L, Mougalian S. Patterns of treatment with everolimus exemestane in hormone receptor-positive HER2-negative metastatic breast cancer in the era of targeted therapy. Breast Cancer Res. 2021;23(1):14. doi: 10.1186/s13058-021-01394-y. - DOI - PMC - PubMed
-
- Di Cosimo S, Sathyanarayanan S, Bendell JC, Cervantes A, Stein MN, Brana I, Roda D, Haines BB, Zhang T, Winter CG, et al. Combination of the mTOR inhibitor ridaforolimus and the anti-IGF1R monoclonal antibody dalotuzumab: preclinical characterization and phase I clinical trial. Clin Cancer Res. 2015;21(1):49–59. doi: 10.1158/1078-0432.CCR-14-0940. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
