

A Pathology-based Case Series of Influenza- and COVID-19-associated Pulmonary Aspergillosis: The Proof Is in the Tissue
- PMID: 37311243
- PMCID: PMC10395719
- DOI: 10.1164/rccm.202208-1570OC
A Pathology-based Case Series of Influenza- and COVID-19-associated Pulmonary Aspergillosis: The Proof Is in the Tissue
Abstract
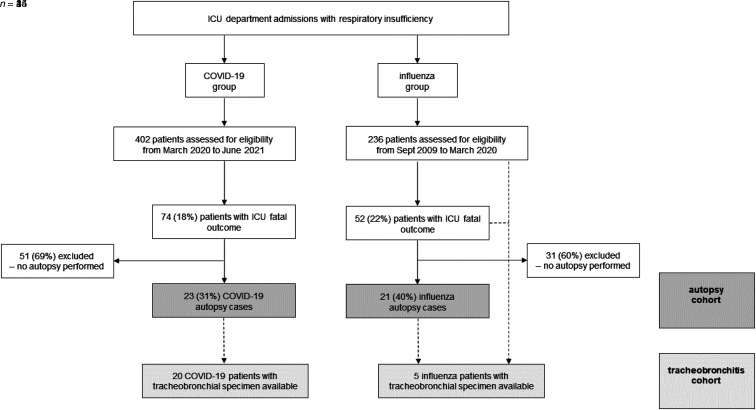
Rationale: Invasive pulmonary aspergillosis has emerged as a frequent coinfection in severe coronavirus disease (COVID-19), similarly to influenza, yet the clinical invasiveness is more debated. Objectives: We investigated the invasive nature of pulmonary aspergillosis in histology specimens of influenza and COVID-19 ICU fatalities in a tertiary care center. Methods: In this monocentric, descriptive, retrospective case series, we included adult ICU patients with PCR-proven influenza/COVID-19 respiratory failure who underwent postmortem examination and/or tracheobronchial biopsy during ICU admission from September 2009 until June 2021. Diagnosis of probable/proven viral-associated pulmonary aspergillosis (VAPA) was made based on the Intensive Care Medicine influenza-associated pulmonary aspergillosis and the European Confederation of Medical Mycology (ECMM) and the International Society for Human and Animal Mycology (ISHAM) COVID-19-associated pulmonary aspergillosis consensus criteria. All respiratory tissues were independently reviewed by two experienced pathologists. Measurements and Main Results: In the 44 patients of the autopsy-verified cohort, 6 proven influenza-associated and 6 proven COVID-19-associated pulmonary aspergillosis diagnoses were identified. Fungal disease was identified as a missed diagnosis upon autopsy in 8% of proven cases (n = 1/12), yet it was most frequently found as confirmation of a probable antemortem diagnosis (n = 11/21, 52%) despite receiving antifungal treatment. Bronchoalveolar lavage galactomannan testing showed the highest sensitivity for VAPA diagnosis. Among both viral entities, an impeded fungal growth was the predominant histologic pattern of pulmonary aspergillosis. Fungal tracheobronchitis was histologically indistinguishable in influenza (n = 3) and COVID-19 (n = 3) cases, yet macroscopically more extensive at bronchoscopy in influenza setting. Conclusions: A proven invasive pulmonary aspergillosis diagnosis was found regularly and with a similar histological pattern in influenza and in COVID-19 ICU case fatalities. Our findings highlight an important need for VAPA awareness, with an emphasis on mycological bronchoscopic work-up.
Keywords: COVID-19; critical illness; histology; human influenza; invasive pulmonary aspergillosis.
Figures
Comment in
-
Viral-associated Pulmonary Aspergillosis: Have We Finally Overcome the Debate of Colonization versus Infection?Am J Respir Crit Care Med. 2023 Aug 1;208(3):230-231. doi: 10.1164/rccm.202306-1022ED. Am J Respir Crit Care Med. 2023. PMID: 37348113 Free PMC article. No abstract available.
References
-
- Schauwvlieghe AFAD, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, Van Tienen C, et al. Dutch-Belgian Mycosis study group Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med . 2018;6:782–792. - PubMed
-
- Vanderbeke L, Janssen NAF, Bergmans DCJJ, Bourgeois M, Buil JB, Debaveye Y, et al. Dutch-Belgian Mycosis Study Group Posaconazole for prevention of invasive pulmonary aspergillosis in critically ill influenza patients (POSA-FLU): a randomised, open-label, proof-of-concept trial. Intensive Care Med . 2021;47:674–686. - PMC - PubMed
-
- Vanderbeke L, Spriet I, Breynaert C, Rijnders BJA, Verweij PE, Wauters J. Invasive pulmonary aspergillosis complicating severe influenza: epidemiology, diagnosis and treatment. Curr Opin Infect Dis . 2018;31:471–480. - PubMed
-
- Nyga R, Maizel J, Nseir S, Chouaki T, Milic I, Roger PA, et al. Invasive tracheobronchial aspergillosis in critically ill patients with severe influenza: a clinical trial. Am J Respir Crit Care Med . 2020;202:708–716. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
