

Breast cancer mortality in 500 000 women with early invasive breast cancer diagnosed in England, 1993-2015: population based observational cohort study
- PMID: 37311588
- PMCID: PMC10261971
- DOI: 10.1136/bmj-2022-074684
Breast cancer mortality in 500 000 women with early invasive breast cancer diagnosed in England, 1993-2015: population based observational cohort study
Erratum in
-
Breast cancer mortality in 500 000 women with early invasive breast cancer in England, 1993-2015: population based observational cohort study.BMJ. 2023 Jul 27;382:p1744. doi: 10.1136/bmj.p1744. BMJ. 2023. PMID: 37500119 Free PMC article. No abstract available.
Abstract
Objectives: To describe long term breast cancer mortality among women with a diagnosis of breast cancer in the past and estimate absolute breast cancer mortality risks for groups of patients with a recent diagnosis.
Design: Population based observational cohort study.
Setting: Routinely collected data from the National Cancer Registration and Analysis Service.
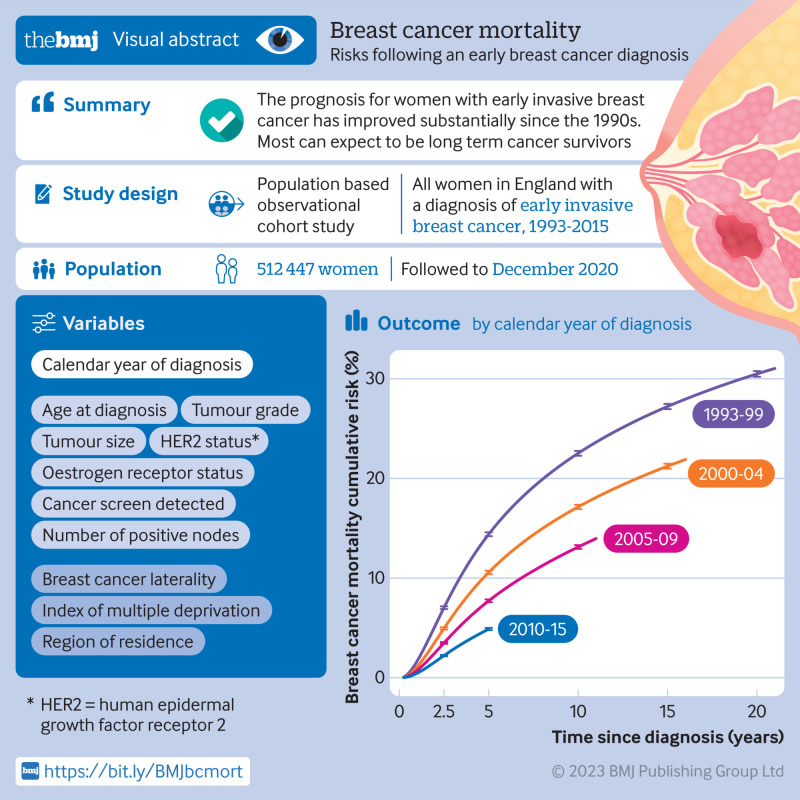
Participants: All 512 447 women registered with early invasive breast cancer (involving only breast and possibly axillary nodes) in England during January 1993 to December 2015, with follow-up to December 2020.
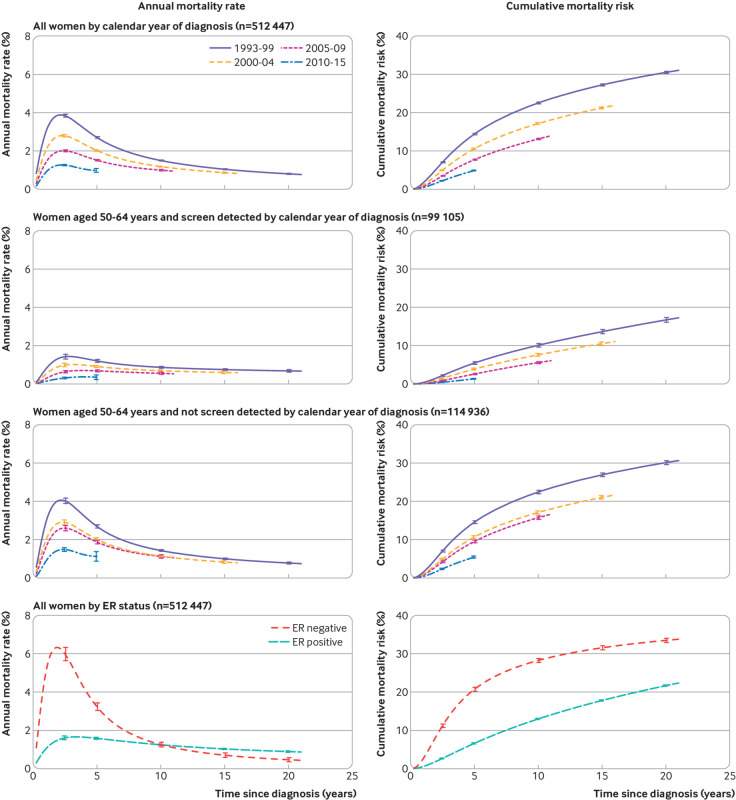
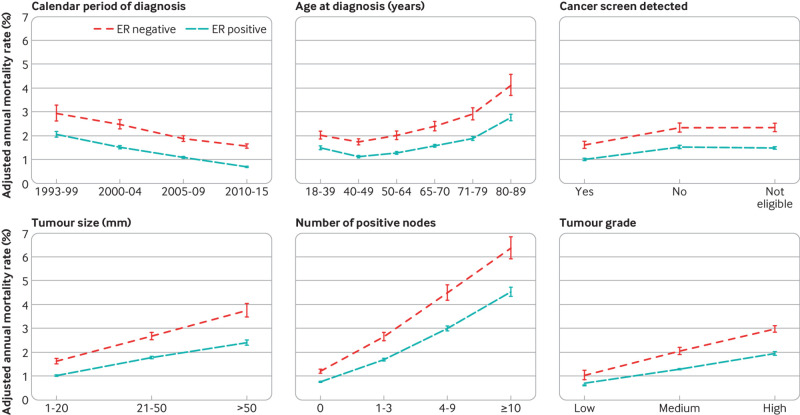
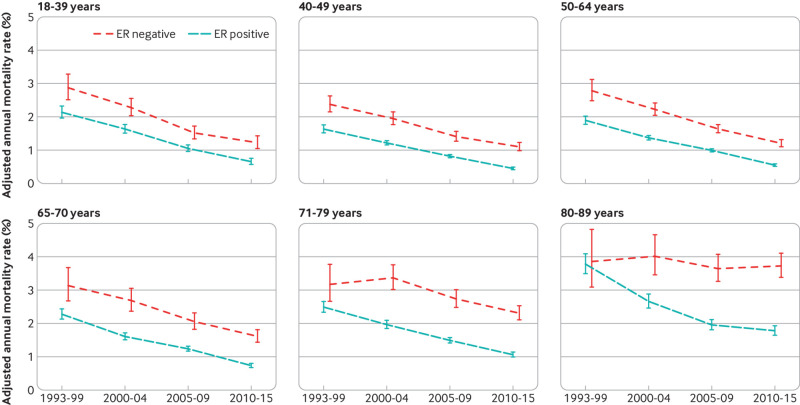
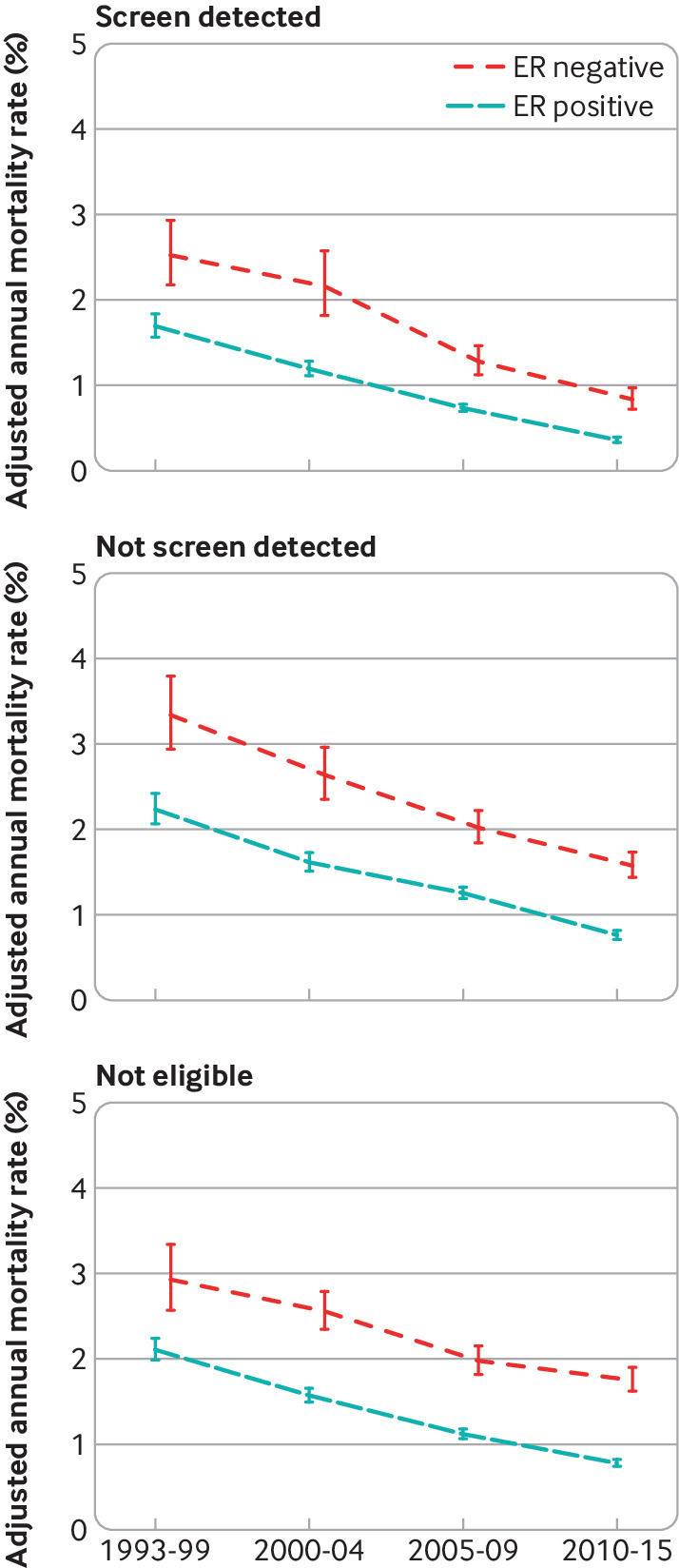
Main outcome measures: Annual breast cancer mortality rates and cumulative risks by time since diagnosis, calendar period of diagnosis, and nine characteristics of patients and tumours.
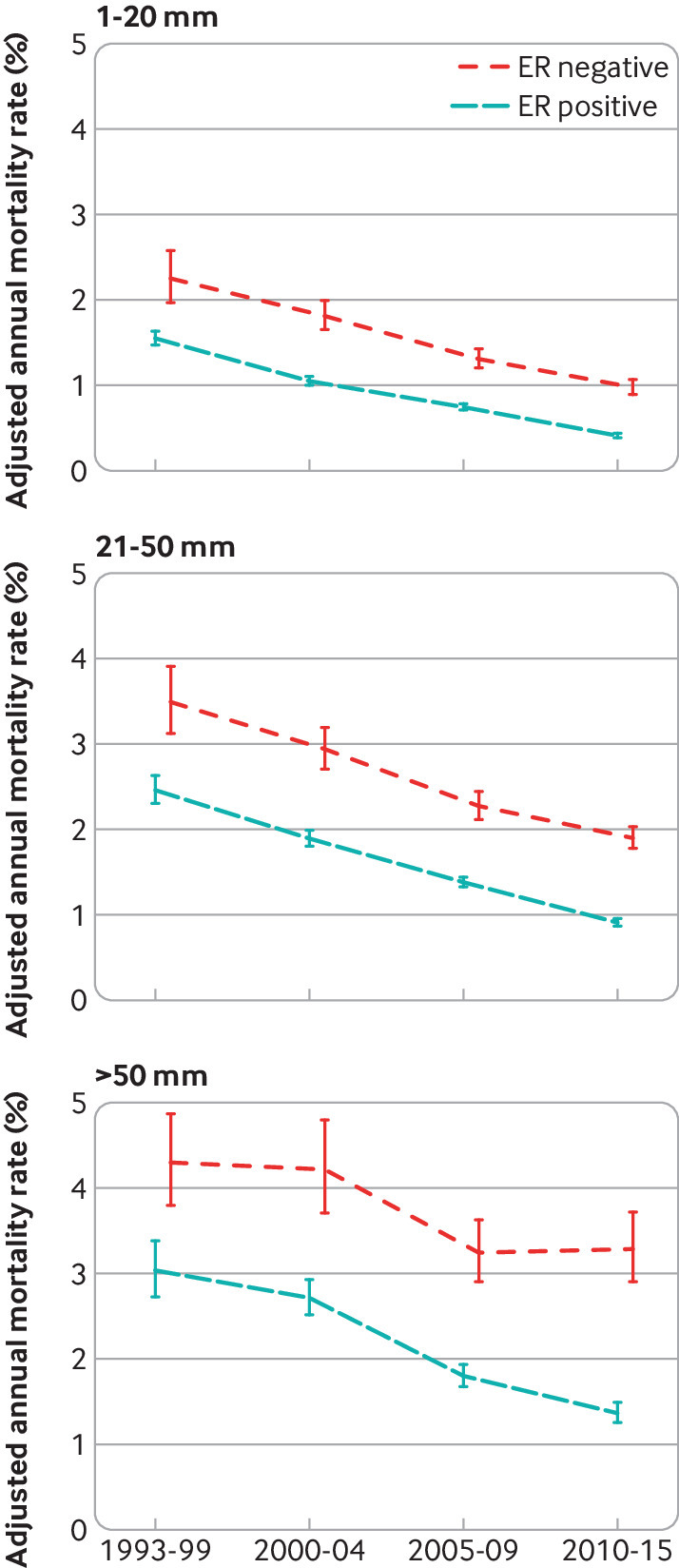
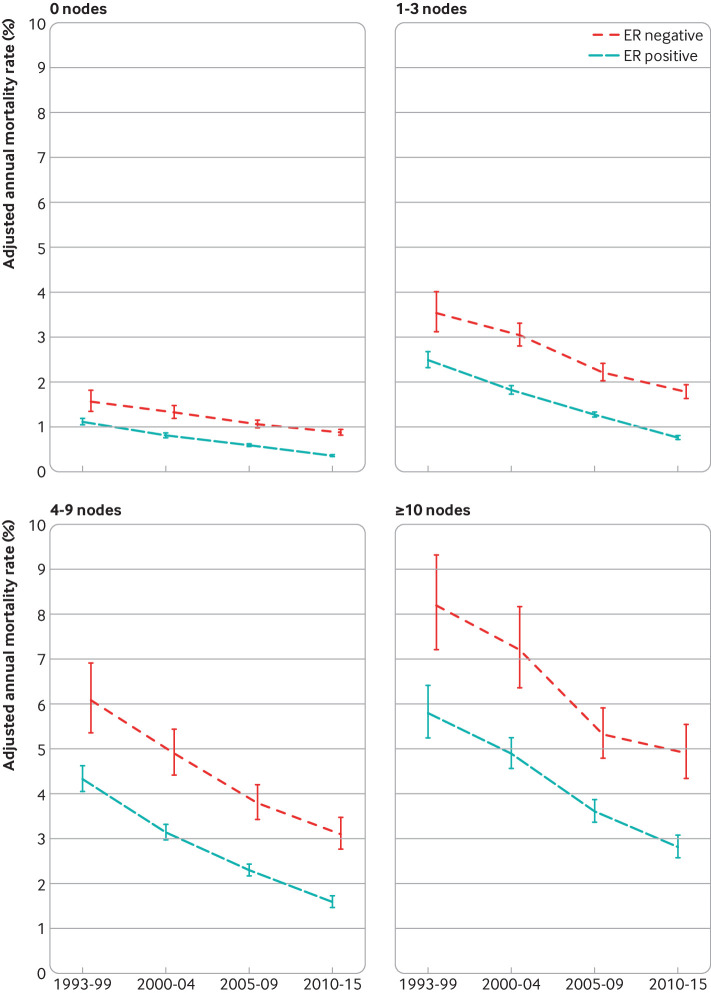
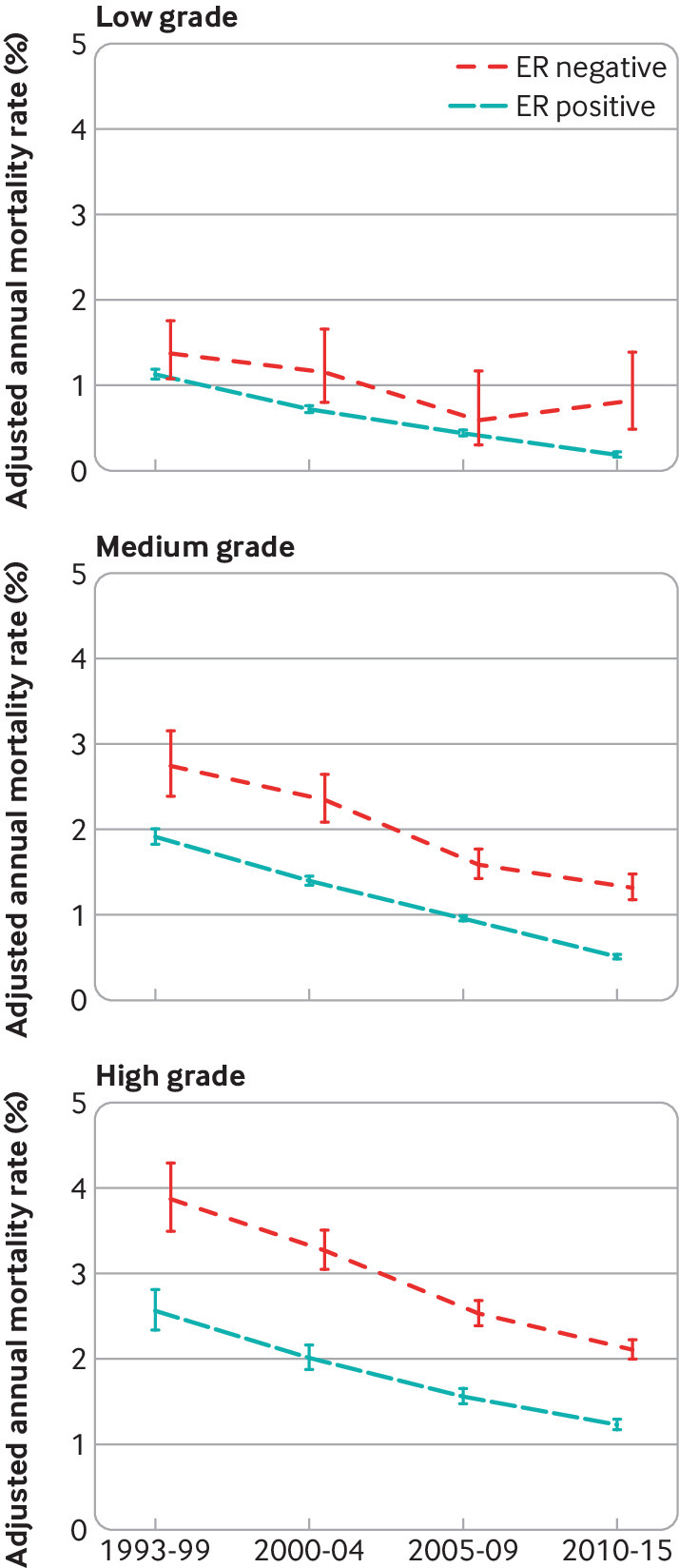
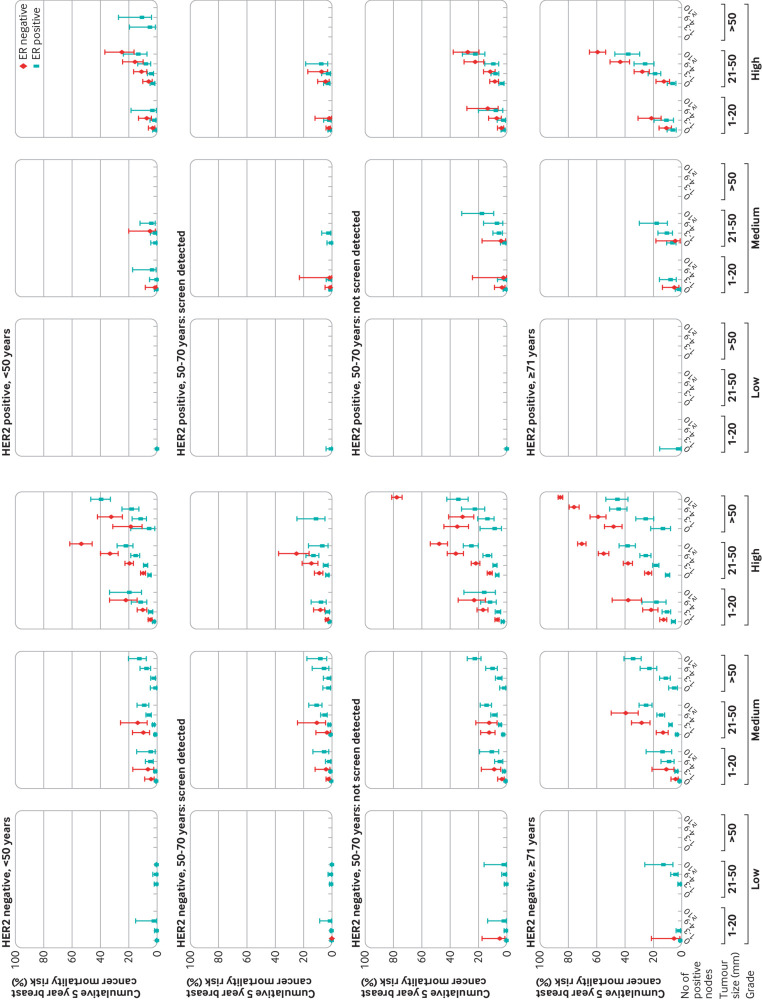
Results: For women with a diagnosis made within each of the calendar periods 1993-99, 2000-04, 2005-09, and 2010-15, the crude annual breast cancer mortality rate was highest during the five years after diagnosis and then declined. For any given time since diagnosis, crude annual breast cancer mortality rates and risks decreased with increasing calendar period. Crude five year breast cancer mortality risk was 14.4% (95% confidence interval 14.2% to 14.6%) for women with a diagnosis made during 1993-99 and 4.9% (4.8% to 5.0%) for women with a diagnosis made during 2010-15. Adjusted annual breast cancer mortality rates also decreased with increasing calendar period in nearly every patient group, by a factor of about three in oestrogen receptor positive disease and about two in oestrogen receptor negative disease. Considering just the women with a diagnosis made during 2010-15, cumulative five year breast cancer mortality risk varied substantially between women with different characteristics: it was <3% for 62.8% (96 085/153 006) of women but ≥20% for 4.6% (6962/153 006) of women.
Conclusions: These five year breast cancer mortality risks for patients with a recent diagnosis may be used to estimate breast cancer mortality risks for patients today. The prognosis for women with early invasive breast cancer has improved substantially since the 1990s. Most can expect to become long term cancer survivors, although for a few the risk remains appreciable.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: support from Cancer Research UK, the National Institute for Health Research Oxford Biomedical Research Centre, the UK Medical Research Council, and the University of Oxford for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Breast cancer: conflating case fatality with mortality.BMJ. 2023 Sep 12;382:2086. doi: 10.1136/bmj.p2086. BMJ. 2023. PMID: 37699614 No abstract available.
References
-
- The International Agency for Research on Cancer. Breast fact sheet. 2020. https://gco.iarc.fr/today/data/factsheets/cancers/20-Breast-fact-sheet.pdf.
-
- van der Meer DJ, Kramer I, van Maaren MC, et al. . Comprehensive trends in incidence, treatment, survival and mortality of first primary invasive breast cancer stratified by age, stage and receptor subtype in the Netherlands between 1989 and 2017. Int J Cancer 2021;148:2289-303. 10.1002/ijc.33417 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous