

Subacute Horizontal Diplopia, Jaw Dystonia, and Laryngospasm
- PMID: 37311643
- PMCID: PMC10265402
- DOI: 10.1212/NXI.0000000000200128
Subacute Horizontal Diplopia, Jaw Dystonia, and Laryngospasm
Erratum in
-
Missing Full Disclosures.Neurol Neuroimmunol Neuroinflamm. 2025 Jan;12(1):e200342. doi: 10.1212/NXI.0000000000200342. Epub 2024 Oct 30. Neurol Neuroimmunol Neuroinflamm. 2025. PMID: 39475708 Free PMC article. No abstract available.
Abstract
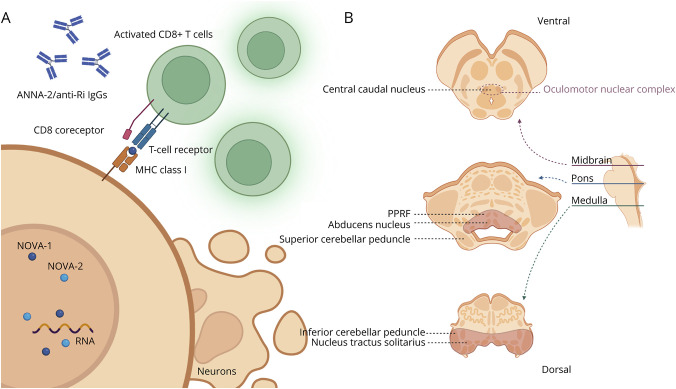
Jaw dystonia and laryngospasm in the context of subacute brainstem dysfunction have been described in a small number of diseases, including antineuronal nuclear antibody type 2 (ANNA-2, also known as anti-Ri) paraneoplastic neurologic syndrome. Severe episodes of laryngospasms causing cyanosis are potentially fatal. Jaw dystonia can also cause eating difficulty, resulting in severe weight loss and malnutrition. In this report, we highlight the multidisciplinary management of this syndrome associated with ANNA-2/anti-Ri paraneoplastic neurologic syndrome and discuss its pathogenesis.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical