

Antibodies Associated With Autoimmune Encephalitis in Patients With Presumed Neurodegenerative Dementia
- PMID: 37311646
- PMCID: PMC10265404
- DOI: 10.1212/NXI.0000000000200137
Antibodies Associated With Autoimmune Encephalitis in Patients With Presumed Neurodegenerative Dementia
Abstract
Background & objectives: Autoimmune encephalitis (AIE) may present with prominent cognitive disturbances without overt inflammatory changes in MRI and CSF. Identification of these neurodegenerative dementia diagnosis mimics is important because patients generally respond to immunotherapy. The objective of this study was to determine the frequency of neuronal antibodies in patients with presumed neurodegenerative dementia and describe the clinical characteristics of the patients with neuronal antibodies.
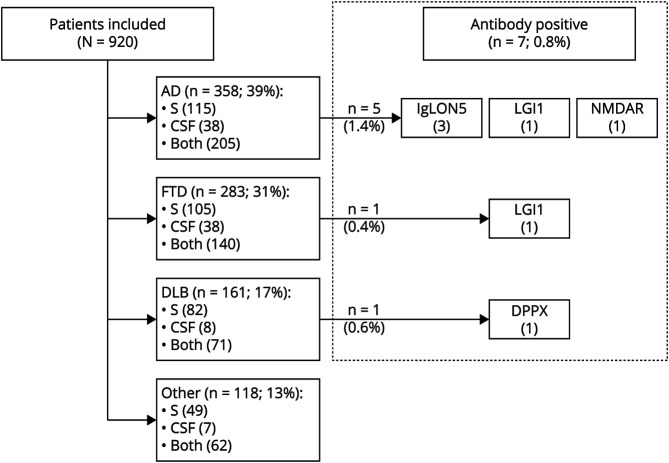
Methods: In this retrospective cohort study, 920 patients were included with neurodegenerative dementia diagnosis from established cohorts at 2 large Dutch academic memory clinics. In total, 1,398 samples were tested (both CSF and serum in 478 patients) using immunohistochemistry (IHC), cell-based assays (CBA), and live hippocampal cell cultures (LN). To ascertain specificity and prevent false positive results, samples had to test positive by at least 2 different research techniques. Clinical data were retrieved from patient files.
Results: Neuronal antibodies were detected in 7 patients (0.8%), including anti-IgLON5 (n = 3), anti-LGI1 (n = 2), anti-DPPX, and anti-NMDAR. Clinical symptoms atypical for neurodegenerative diseases were identified in all 7 and included subacute deterioration (n = 3), myoclonus (n = 2), a history of autoimmune disease (n = 2), a fluctuating disease course (n = 1), and epileptic seizures (n = 1). In this cohort, no patients with antibodies fulfilled the criteria for rapidly progressive dementia (RPD), yet a subacute deterioration was reported in 3 patients later in the disease course. Brain MRI of none of the patients demonstrated abnormalities suggestive for AIE. CSF pleocytosis was found in 1 patient, considered as an atypical sign for neurodegenerative diseases. Compared with patients without neuronal antibodies (4 per antibody-positive patient), atypical clinical signs for neurodegenerative diseases were seen more frequently among the patients with antibodies (100% vs 21%, p = 0.0003), especially a subacute deterioration or fluctuating course (57% vs 7%, p = 0.009).
Discussion: A small, but clinically relevant proportion of patients suspected to have neurodegenerative dementias have neuronal antibodies indicative of AIE and might benefit from immunotherapy. In patients with atypical signs for neurodegenerative diseases, clinicians should consider neuronal antibody testing. Physicians should keep in mind the clinical phenotype and confirmation of positive test results to avoid false positive results and administration of potential harmful therapy for the wrong indication.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
A.E.M. Bastiaansen reports no disclosures. R.W. van Steenhoven reports no disclosures. Research programs of Wiesje van der Flier have been funded by ZonMW, now, EUFP7, EU-JPND, Alzheimer Nederland, Hersenstichting CardioVascular Onderzoek Nederland, Health∼Holland, Topsector Life Sciences & Health, stichting Dioraphte, Gieskes-Strijbis fonds, stichting Equilibrio, Edwin Bouw fonds, Pasman stichting, stichting Alzheimer & Neuropsychiatrie Foundation, Philips, Biogen MA Inc, Novartis-NL, Life-MI, AVID, Roche BV, Fujifilm, and Combinostics. W.M. van der Flier holds the Pasman chair. W.M. van der Flier is recipient of ABOARD, which is a public-private partnership receiving funding from ZonMW (#73305095007) and Health Holland, Topsector Life Sciences & Health (PPP-allowance; #LSHM20106). All funding is paid to her institution. WF has performed contract research for Biogen MA Inc and Boehringer Ingelheim. All funding is paid to her institution. W.M. van der Flier has been an invited speaker at Boehringer Ingelheim, Biogen MA Inc, Danone, Eisai, WebMD Neurology (Medscape), and Springer Healthcare. All funding is paid to her institution. W.M. van der Flier is consultant to Oxford Health Policy Forum CIC, Roche, and Biogen MA Inc. All funding is paid to her institution. W.M. van der Flier participated in advisory boards of Biogen MA Inc and Roche. All funding is paid to her institution. W.M. van der Flier is a member of the steering committee of PAVE and Think Brain Health. W.M. van der Flier was an associate editor of Alzheimer, Research & Therapy in 2020/2021. W.M. van der Flier is an associate editor at Brain. Research of C. Teunissen was supported by the European Commission (Marie Curie International Training Network, Grant Agreement No. 860197 (MIRIADE)), Innovative Medicines Initiatives 3TR (Horizon 2020, Grant No. 831434), EPND (IMI 2 Joint Undertaking (JU) under Grant Agreement No. 101034344) and JPND (bPRIDE), National MS Society (Progressive MS alliance) and Health Holland, the Dutch Research Council (ZonMW), Alzheimer Drug Discovery Foundation, The Selfridges Group Foundation, Alzheimer Netherlands, and Alzheimer Association. C. Teunissen is recipient of ABOARD, which is a public-private partnership receiving funding from ZonMW (#73305095007) and Health∼Holland, Topsector Life Sciences & Health (PPP-allowance, #LSHM20106). ABOARD also receives funding from Edwin Bouw Fonds and Gieskes-Strijbisfonds. C. Teunissen has a collaboration contract with ADx Neurosciences, Quanterix, and Eli Lilly, performed contract research or received grants from AC-Immune, Axon Neurosciences, Bioconnect, Bioorchestra, Brainstorm Therapeutics, Celgene, EIP Pharma, Eisai, Grifols, Novo Nordisk, PeopleBio, Roche, Toyama, and Vivoryon. She serves on editorial boards of Medidact Neurologie/Springer, Alzheimer Research and Therapy, and Neurology: Neuroimmunology & Neuroinflammation and is an editor of a Neuromethods book Springer. She had speaker contracts for Roche, Grifols, and Novo Nordisk. E. de Graaff holds a patent for the detection of anti-DNER antibodies. M.M.P. Nagtzaam reports no disclosures. M. Paunovic reports no disclosures. S. Franken reports no disclosures. M.W.J. Schreurs reports no disclosures. F. Leypoldt has received speakers honoraria from Grifols, Roche, Novartis, Alexion, and Biogen and serves on an advisory board for Roche and Biogen. He works for an academic institution (University Hospital Schleswig-Holstein) which offers commercial autoantibody testing. P.A.E. Sillevis Smitt holds a patent for the detection of anti-DNER and received research support from Euroimmun. J.M. de Vries reports no disclosures. H. Seelaar reports no disclosures. J.C. van Swieten reports no disclosures. F.J. de Jong reports no disclosures. Y.A.L. Pijnenburg Research of Alzheimer center Amsterdam is part of the neurodegeneration research program of Amsterdam Neuroscience. Alzheimer Center Amsterdam is supported by Stichting Alzheimer Nederland and Stichting VUmc fonds. The chair of Wiesje van der Flier is supported by the Pasman stichting. M.J. Titulaer has filed a patent, on behalf of the Erasmus MC, for methods for typing neurologic disorders and cancer, and devices for use therein, and has received research funds for serving on a scientific advisory board of Horizon Therapeutics, for consultation at Guidepoint Global LLC, for consultation at UCB, for teaching colleagues by Novartis. MT has received an unrestricted research grant from Euroimmun AG and from CSL Behring. Go to
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical