

Reduced side effects and improved pain management by continuous ketorolac infusion with patient-controlled fentanyl injection compared with single fentanyl administration in pelviscopic gynecologic surgery: a randomized, double-blind, controlled study
- PMID: 37312413
- PMCID: PMC10834721
- DOI: 10.4097/kja.23217
Reduced side effects and improved pain management by continuous ketorolac infusion with patient-controlled fentanyl injection compared with single fentanyl administration in pelviscopic gynecologic surgery: a randomized, double-blind, controlled study
Abstract
Background: A combination of opioids and adjunctive drugs can be used for intravenous patient-controlled analgesia (PCA) to minimize opioid-related side effects. We investigated whether two different analgesics administered separately via a dual-chamber PCA have fewer side effects with adequate analgesia than a single fentanyl PCA in gynecologic pelviscopic surgery.
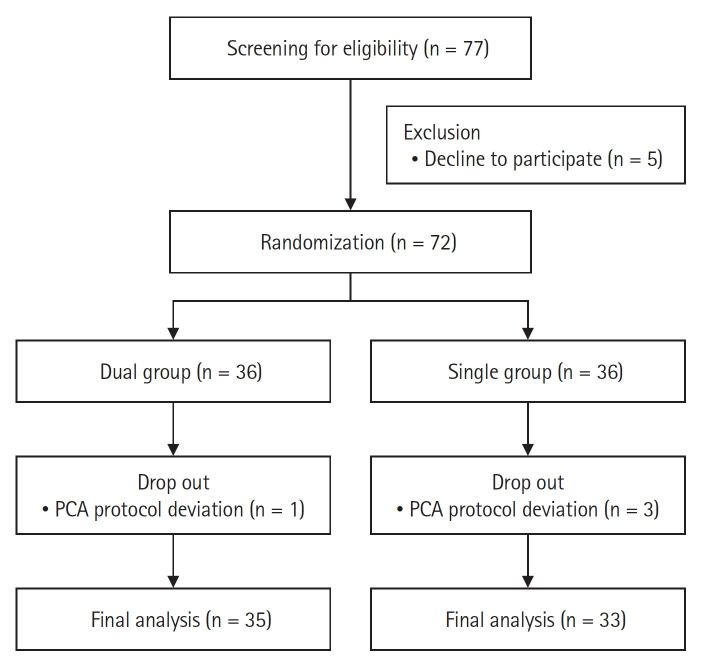
Methods: This prospective, double-blind, randomized, and controlled study included 68 patients who underwent pelviscopic gynecological surgery. Patients were allocated to either the dual (ketorolac and fentanyl delivered by a dual-chamber PCA) or the single (fentanyl alone) group. Postoperative nausea and vomiting (PONV) and analgesic quality were compared between the two groups at 2, 6, 12, and 24 h postoperatively.
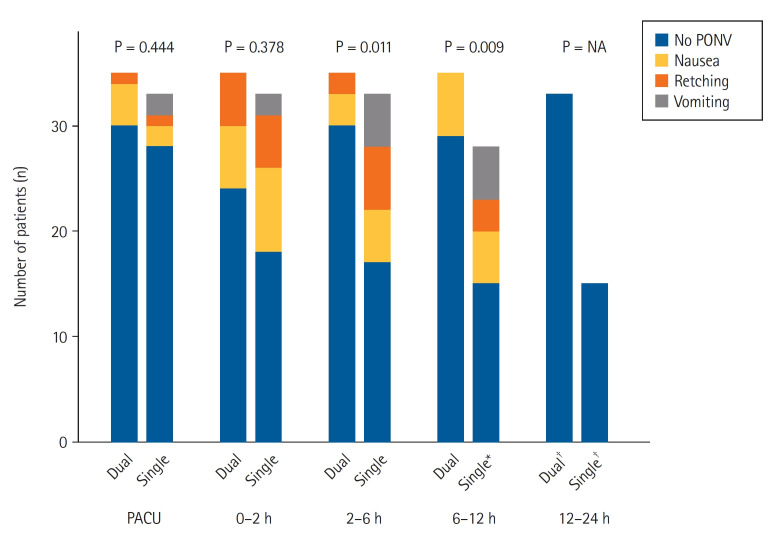
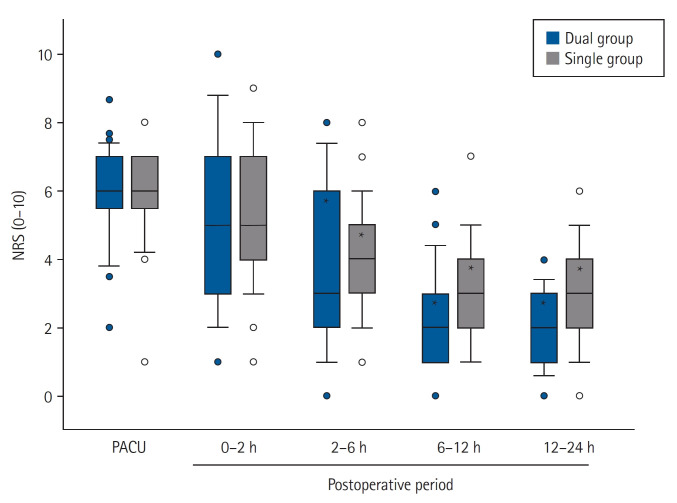
Results: The dual group showed a significantly lower incidence of PONV during postoperative 2-6 h (P = 0.011) and 6-12 h (P = 0.009). Finally, only two patients (5.7%) in the dual group and 18 (54.5%) in the single group experienced PONV during the entire postoperative 24 h and could not maintain intravenous PCA (odds ratio: 0.056, 95% CI [0.007, 0.229], P < 0.001). Despite the administration of less fentanyl via intravenous PCA during the postoperative 24 h in the dual group than in the single group (66.0 ± 77.8 vs. 383.6 ± 70.1 μg, P < 0.001), postoperative pain had no significant intergroup difference.
Conclusions: Two different analgesics, continuous ketorolac and intermittent fentanyl bolus, administered via dual-chamber intravenous PCA, showed fewer side effects with adequate analgesia than conventional intravenous fentanyl PCA in gynecologic patients undergoing pelviscopic surgery.
Keywords: Analgesia; Fentanyl; Ketorolac; Patient-controlled analgesia; Postoperative nausea and vomiting; Postoperative pain.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Effect of patient-controlled analgesia on development of postoperative nausea and vomiting in patients undergoing microvascular decompression: a prospective randomized controlled trial.J Neurosurg. 2024 Feb 9;141(1):260-267. doi: 10.3171/2023.12.JNS231817. Print 2024 Jul 1. J Neurosurg. 2024. PMID: 38335521 Clinical Trial.
-
Dexmedetomidine added to an opioid-based analgesic regimen for the prevention of postoperative nausea and vomiting in highly susceptible patients: A randomised controlled trial.Eur J Anaesthesiol. 2016 Feb;33(2):75-83. doi: 10.1097/EJA.0000000000000327. Eur J Anaesthesiol. 2016. PMID: 26258655 Clinical Trial.
-
Effect of Dexmedetomidine Alone for Intravenous Patient-Controlled Analgesia After Gynecological Laparoscopic Surgery: A Consort-Prospective, Randomized, Controlled Trial.Medicine (Baltimore). 2016 May;95(19):e3639. doi: 10.1097/MD.0000000000003639. Medicine (Baltimore). 2016. PMID: 27175680 Free PMC article. Clinical Trial.
-
[Intravenous patient-controlled analgesia (IV-PCA) for relief of postoperative pain].Masui. 2011 Aug;60(8):908-12. Masui. 2011. PMID: 21861414 Review. Japanese.
-
Optimizing patient-controlled analgesia: a narrative review based on a single center audit process.Anesth Pain Med (Seoul). 2024 Jul;19(3):171-184. doi: 10.17085/apm.24075. Epub 2024 Jul 31. Anesth Pain Med (Seoul). 2024. PMID: 39118331 Free PMC article. Review.
Cited by
-
Physicochemical stability of mixtures of non-steroidal anti-inflammatory drugs such as ketorolac and diclofenac and antiemetics such as ondansetron and ramosetron: an in vitro study.Korean J Pain. 2025 Apr 1;38(2):103-115. doi: 10.3344/kjp.24316. Korean J Pain. 2025. PMID: 40159937 Free PMC article.
-
Analysis of the effect of fentanyl dosage used in patient-controlled analgesia for pain management after oral cancer surgery: a retrospective observational study.J Dent Anesth Pain Med. 2025 Feb;25(1):43-53. doi: 10.17245/jdapm.2025.25.1.43. Epub 2025 Jan 22. J Dent Anesth Pain Med. 2025. PMID: 39944845 Free PMC article.
References
-
- Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87:36–46. - PubMed
-
- Rawal N. Current issues in postoperative pain management. Eur J Anaesthesiol. 2016;33:160–71. - PubMed
-
- Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–20. - PubMed
-
- Peduto VA, Ballabio M, Stefanini S. Efficacy of propacetamol in the treatment of postoperative pain. Morphine-sparing effect in orthopedic surgery. Italian Collaborative Group on Propacetamol. Acta Anaesthesiol Scand. 1998;42:293–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
