

Prediction of local recurrence in tenosynovial giant cell tumor of the knee: Based on preoperative MRI evaluation into disease subtypes and severity
- PMID: 37315053
- PMCID: PMC10266632
- DOI: 10.1371/journal.pone.0287028
Prediction of local recurrence in tenosynovial giant cell tumor of the knee: Based on preoperative MRI evaluation into disease subtypes and severity
Abstract
Objective: Tenosynovial giant cell tumors (TSGCTs) of the knee differ in their clinical outcome according to disease subtypes and severity. The aim of this study was to determine the predictive MRI features related to local recurrence in TSGCT of the knee regarding disease subtypes and severity.
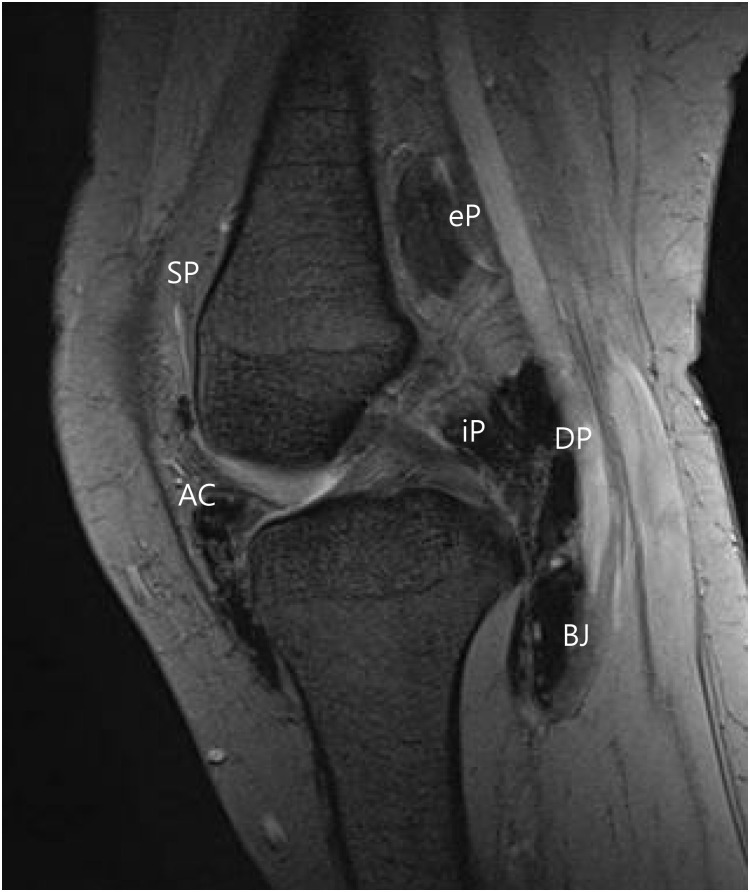
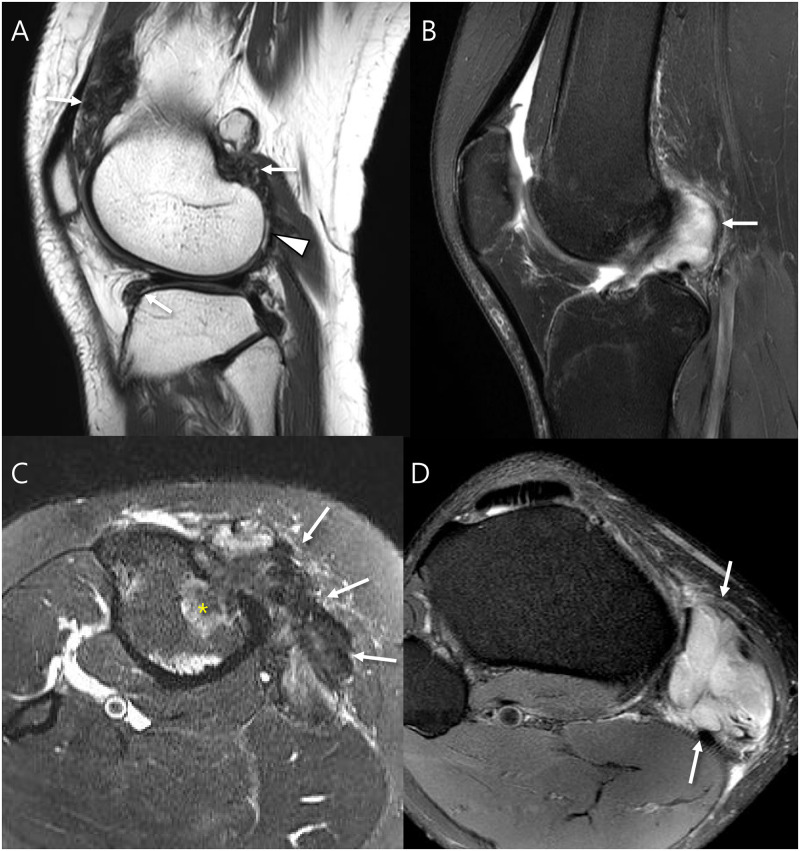
Methods: This retrospective study included 20 patients with pathology-proven TSGCT of the knee who underwent preoperative MRI and surgery from Jan. 2007 to Jan. 2022. The anatomical point of the lesion was determined with a knee mapping. And then MRI features related to disease subtype including nodularity (single vs. multinodular); margin (circumscribed vs. infiltrative); peripheral hypointenseity (present vs. absent); internal hypointensity reflecting hemosiderin deposition (speckled vs. granular) were assessed. Third, MRI features related to disease severity including involvement of bone, cartilage, and tendon were evaluated. MRI features for predicting local recurrence of TSGCT were tested using chi-square test and logistic regression analysis.
Results: Ten patients with diffuse-type TSGCT (D-TSGCT) and 10 patients with localized-type TSGCT (L-TSGCT) were included. There were six cases of local recurrence and all of them were D-TSGCT and none for L-TSGCT with statistical difference (P = 0.015). D-TSGCT that was direct risk factor for local recurrence showed more multinodular (80.0% vs. 10.0%; P = 0.007), infiltrative margin (90.0% vs. 10.0%; P = 0.002), and absent peripheral hypointensity (100.0% vs. 20.0%; P = 0.001) than L-TSGCT. Multivariate analysis showed infiltrative margin (odds ratio [OR], 81.0; P = 0.003) was independent MRI factor for D-TSGCT. Disease severity for risk of local recurrence included cartilage (66.7% vs. 7.1%; P = 0.024) and tendon (100.0% vs. 28.6%; P = 0.015) involvement compared to no local recurrence. Multivariate analysis showed tendon involvement (OR, 12.5; P = 0.042) was predictive MRI parameter for local recurrence. By combining tumor margin and tendon involvement, local recurrence was predicted sensitively on preoperative MRI (sensitivity, 100%; specificity, 50%; accuracy, 65%).
Conclusion: D-TSGCTs was associated with local recurrence and showed multinodularity infiltrative margin, and absent peripheral hypointensity. Disease severity including cartilage and tendon involvement was associated with local recurrence. Preoperative MRI evaluation by combining disease subtypes and severity can predict local recurrence sensitively.
Copyright: © 2023 Kim et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Diffuse-Type Tenosynovial Giant Cell Tumor: What Are the Important Findings on the Initial and Follow-Up MRI?Cancers (Basel). 2024 Jan 17;16(2):402. doi: 10.3390/cancers16020402. Cancers (Basel). 2024. PMID: 38254890 Free PMC article. Review.
-
MRI Prediction Model for Tenosynovial Giant Cell Tumor with Risk of Diffuse-type.Acad Radiol. 2023 Nov;30(11):2616-2624. doi: 10.1016/j.acra.2023.01.012. Epub 2023 Feb 6. Acad Radiol. 2023. PMID: 36754646
-
Tenosynovial giant cell tumors of digits: MRI differentiation between localized types and diffuse types with pathology correlation.Skeletal Radiol. 2023 Mar;52(3):593-603. doi: 10.1007/s00256-022-04170-x. Epub 2022 Sep 5. Skeletal Radiol. 2023. PMID: 36063189
-
Diffuse type tenosynovial giant cell tumour in the sinus tarsi in a paediatric patient: a rare case report with radiological and histopathological analysis.Skeletal Radiol. 2025 Aug;54(8):1773-1778. doi: 10.1007/s00256-025-04905-6. Epub 2025 Mar 13. Skeletal Radiol. 2025. PMID: 40080140
-
Optimal Treatment for Tenosynovial Giant Cell Tumor of the Hand.J Nippon Med Sch. 2020 Sep 9;87(4):184-190. doi: 10.1272/jnms.JNMS.2020_87-408. Epub 2020 Apr 30. J Nippon Med Sch. 2020. PMID: 32350187 Review.
Cited by
-
Arthroscopic Excision of a Localized Tenosynovial Giant Cell Tumor of the Knee: A Case Report.Curr Rheumatol Rev. 2024;20(4):459-464. doi: 10.2174/0115733971272967231120114621. Curr Rheumatol Rev. 2024. PMID: 38231053
-
Diffuse-Type Tenosynovial Giant Cell Tumor: What Are the Important Findings on the Initial and Follow-Up MRI?Cancers (Basel). 2024 Jan 17;16(2):402. doi: 10.3390/cancers16020402. Cancers (Basel). 2024. PMID: 38254890 Free PMC article. Review.
-
Cytoplasmic PPARγ Significantly Correlates With P53 Immunohistochemical Expression and Tumor Size in Localized Tenosynovial Giant Cell Tumor.Cureus. 2024 May 15;16(5):e60377. doi: 10.7759/cureus.60377. eCollection 2024 May. Cureus. 2024. PMID: 38882990 Free PMC article.
References
-
- Fletcher CDM. WHO classification of tumours of soft tissue and bone. 2013:281–95.
-
- Ehrenstein V, Andersen SL, Qazi I, Sankar N, Pedersen AB, Sikorski R, et al.. Tenosynovial Giant Cell Tumor: Incidence, Prevalence, Patient Characteristics, and Recurrence. A Registry-based Cohort Study in Denmark. The Journal of rheumatology. 2017;44(10):1476–83. Epub 2017/08/03. doi: 10.3899/jrheum.160816 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
