

Gut microbiome composition may be an indicator of preclinical Alzheimer's disease
- PMID: 37315112
- PMCID: PMC10680783
- DOI: 10.1126/scitranslmed.abo2984
Gut microbiome composition may be an indicator of preclinical Alzheimer's disease
Abstract
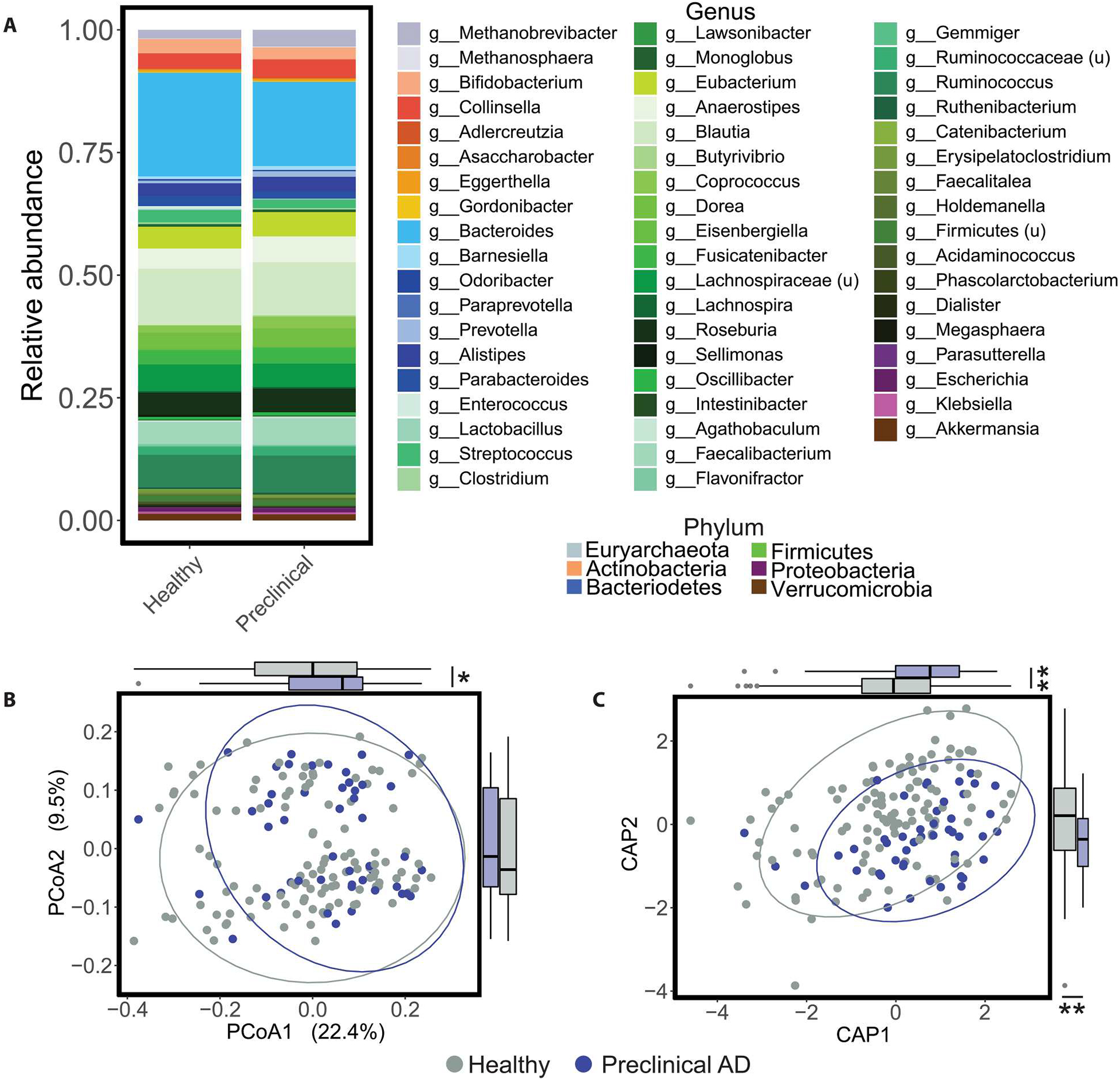
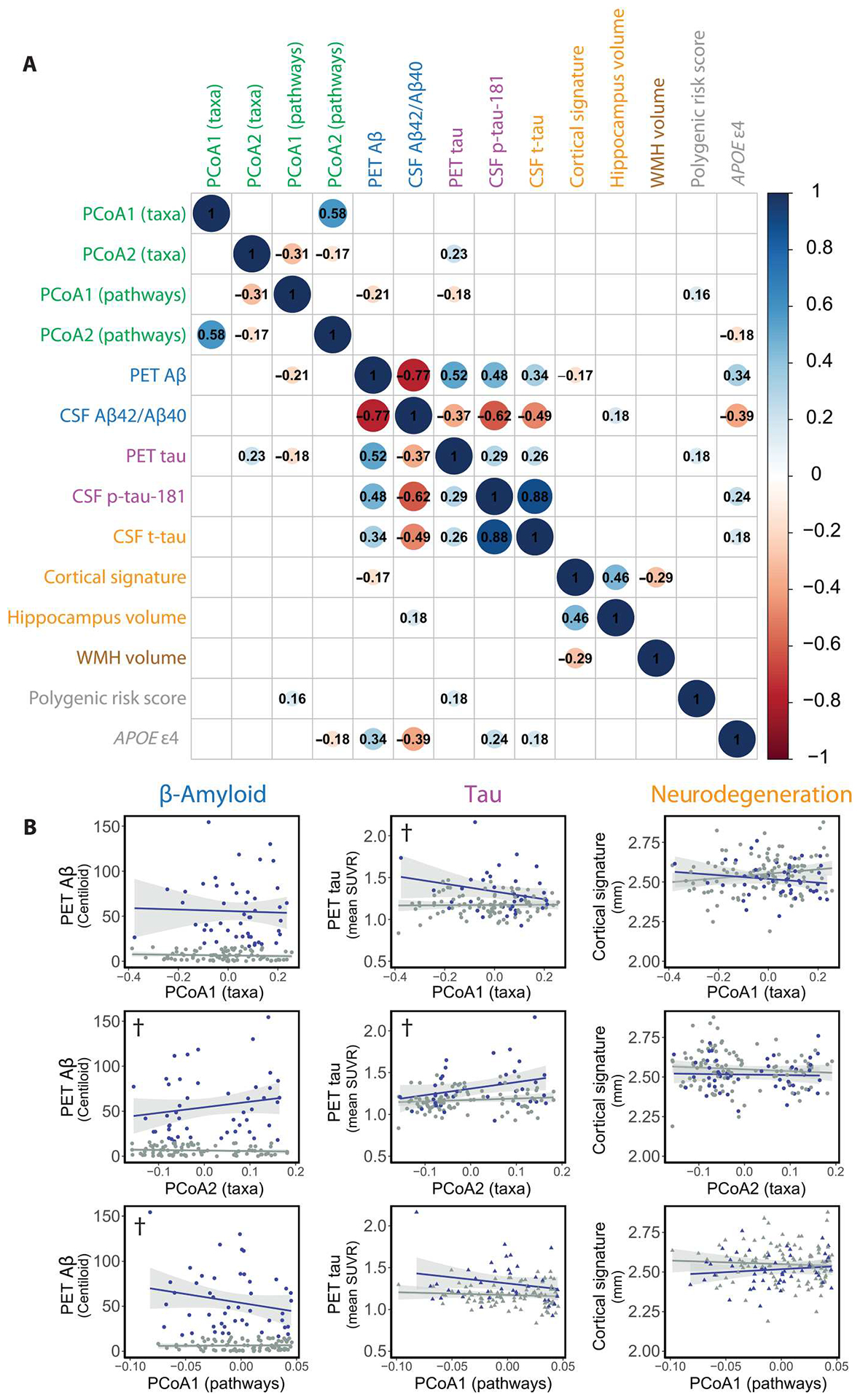
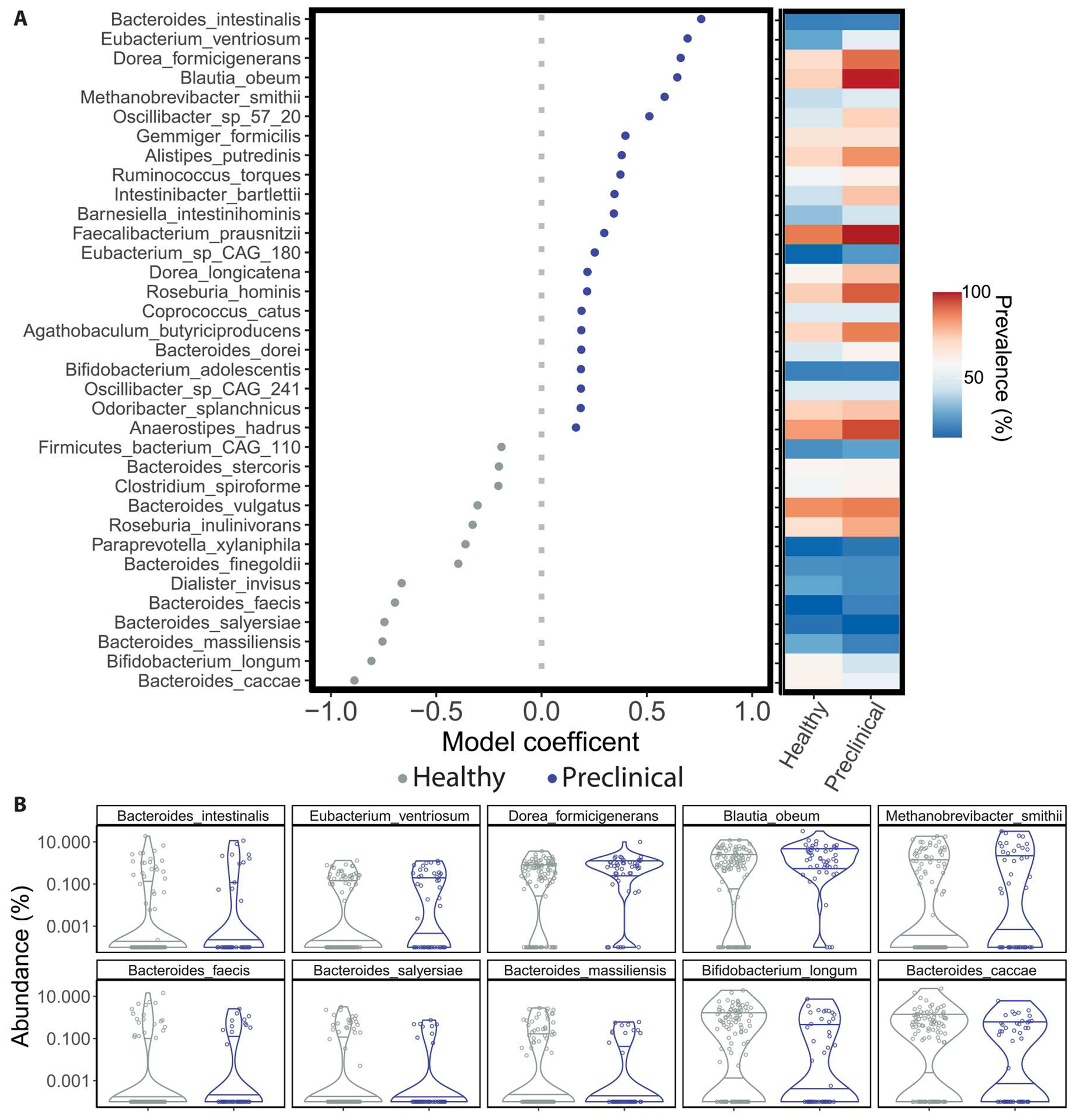
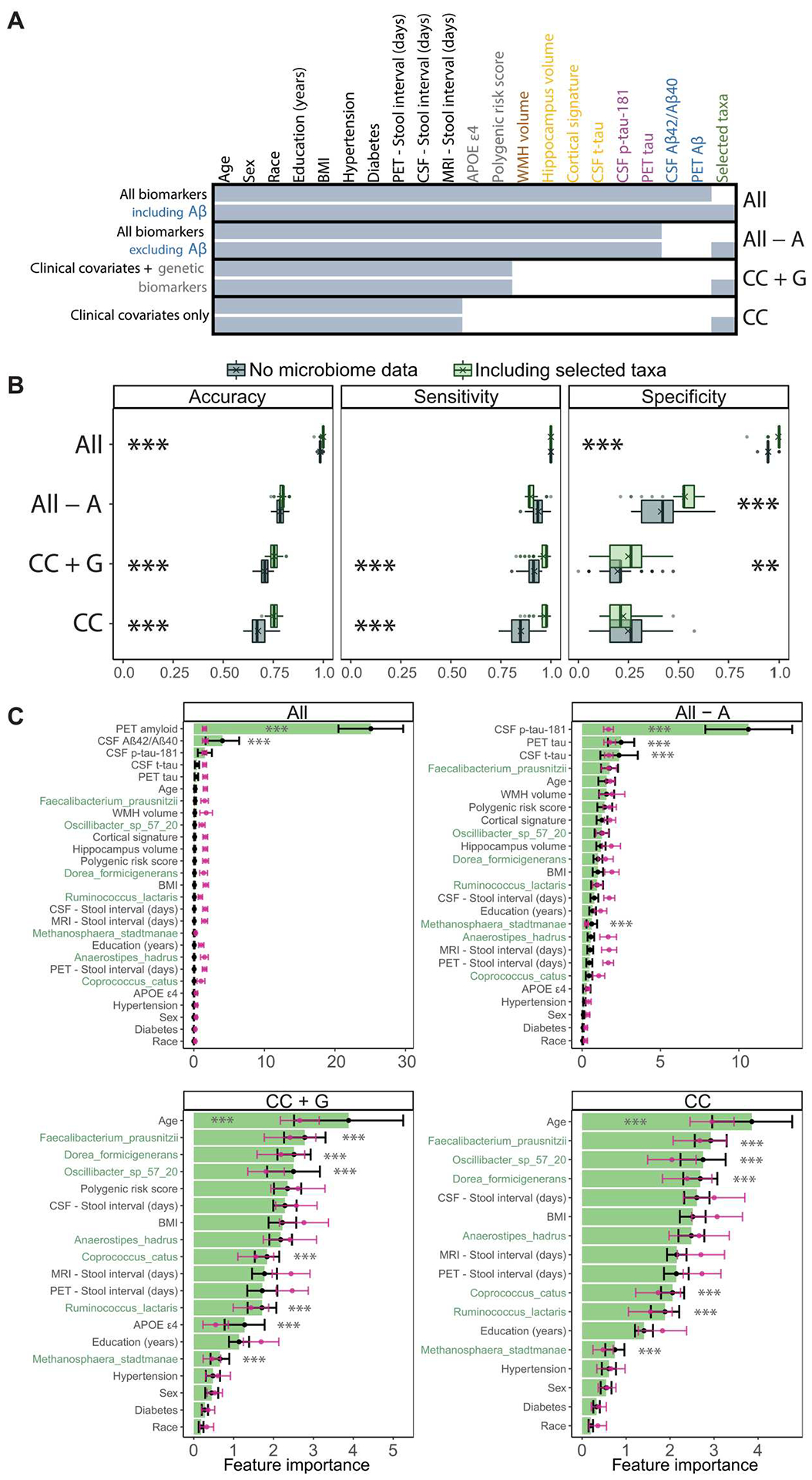
Alzheimer's disease (AD) pathology is thought to progress from normal cognition through preclinical disease and ultimately to symptomatic AD with cognitive impairment. Recent work suggests that the gut microbiome of symptomatic patients with AD has an altered taxonomic composition compared with that of healthy, cognitively normal control individuals. However, knowledge about changes in the gut microbiome before the onset of symptomatic AD is limited. In this cross-sectional study that accounted for clinical covariates and dietary intake, we compared the taxonomic composition and gut microbial function in a cohort of 164 cognitively normal individuals, 49 of whom showed biomarker evidence of early preclinical AD. Gut microbial taxonomic profiles of individuals with preclinical AD were distinct from those of individuals without evidence of preclinical AD. The change in gut microbiome composition correlated with β-amyloid (Aβ) and tau pathological biomarkers but not with biomarkers of neurodegeneration, suggesting that the gut microbiome may change early in the disease process. We identified specific gut bacterial taxa associated with preclinical AD. Inclusion of these microbiome features improved the accuracy, sensitivity, and specificity of machine learning classifiers for predicting preclinical AD status when tested on a subset of the cohort (65 of the 164 participants). Gut microbiome correlates of preclinical AD neuropathology may improve our understanding of AD etiology and may help to identify gut-derived markers of AD risk.
Conflict of interest statement
G.D. is a co-founder, holder of equity in, a consultant to, and a member of the Scientific Advisory Board of Viosera Therapeutics, which is developing combination antimicrobial therapy against bacterial pathogens. G.D. is a co-inventor on a patent assigned to Viosera Therapeutics. G.D. is a consultant to and a member of the Scientific Advisory Board of Pluton Biosciences and has consulted for SNIPR Technologies Ltd. in the last 5 years. P.I.T. is a holder of equity in, a consultant to, and a member of the Scientific Advisory Board of MediBeacon Inc. and is a co-inventor on patents assigned to MediBeacon; Chair of the Scientific Advisory Board of the AGA Center for Microbiome Research and Education (a paid position); a consultant to Temple University on waterborne enteric infections; a recipient of royalties from UpToDate; and an unpaid member of the Data Safety Monitoring Board of Inmunova. D.M.H. co-founded and is on the Scientific Advisory Board of C2N Diagnostics and consults for Genentech, Denali, Cajal Neurosciences, C2N Diagnostics, and Asteroid. Washington University receives research grants to the laboratory of D.M.H. from NextCure, Eli Lilly, Novartis, Ionis, and Denali. T.L.S.B. receives research funding from Siemens as well as technical support and materials from Avid Radiopharmaceuticals, Cerveau, and Life Molecular Imaging. T.L.S.B. also receives paid and unpaid consulting and has advisory roles for Siemens, Eli Lilly, Roche, Life Molecular Imaging, Biogen, and Eisai. A.M.F. was a member of the scientific advisory boards for Roche Diagnostics, Genentech, and Diadem and also previously consulted for DiamiR and Siemens Healthcare Diagnostics Inc. S.E.S. has analyzed data provided by C2N Diagnostics to Washington University and has served on a Scientific Advisory Board for Eisai. C.C. has received research support from GlaxoSmithKline and Eisai and is a member of the advisory board of Vivid Genomics and Circular Genomics and owns stocks. J.C.M. is a member of the Barcelona Brain Research Foundation Scientific Advisory Board, the Native Alzheimer Disease-Related Resource Center in Minority Aging Research External Advisory Board, the Cure Alzheimer’s Fund Research Strategy Council, and the Longer Life Foundation Board of Governors. J.C.M. was previously a member of the Diverse VCID (Vascular Contributions to Cognitive Impairment and Dementia) Observational Study Monitoring Board.
Figures
Comment in
-
Early microbiome changes in neurodegenerative disease.Nat Rev Neurol. 2023 Aug;19(8):458. doi: 10.1038/s41582-023-00848-5. Nat Rev Neurol. 2023. PMID: 37402802 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
