

Rapid reduction in Staphylococcus aureus in atopic dermatitis subjects following dupilumab treatment
- PMID: 37315812
- PMCID: PMC10716365
- DOI: 10.1016/j.jaci.2023.05.026
Rapid reduction in Staphylococcus aureus in atopic dermatitis subjects following dupilumab treatment
Abstract
Background: Atopic dermatitis (AD) is an inflammatory disorder characterized by dominant type 2 inflammation leading to chronic pruritic skin lesions, allergic comorbidities, and Staphylococcus aureus skin colonization and infections. S aureus is thought to play a role in AD severity.
Objectives: This study characterized the changes in the host-microbial interface in subjects with AD following type 2 blockade with dupilumab.
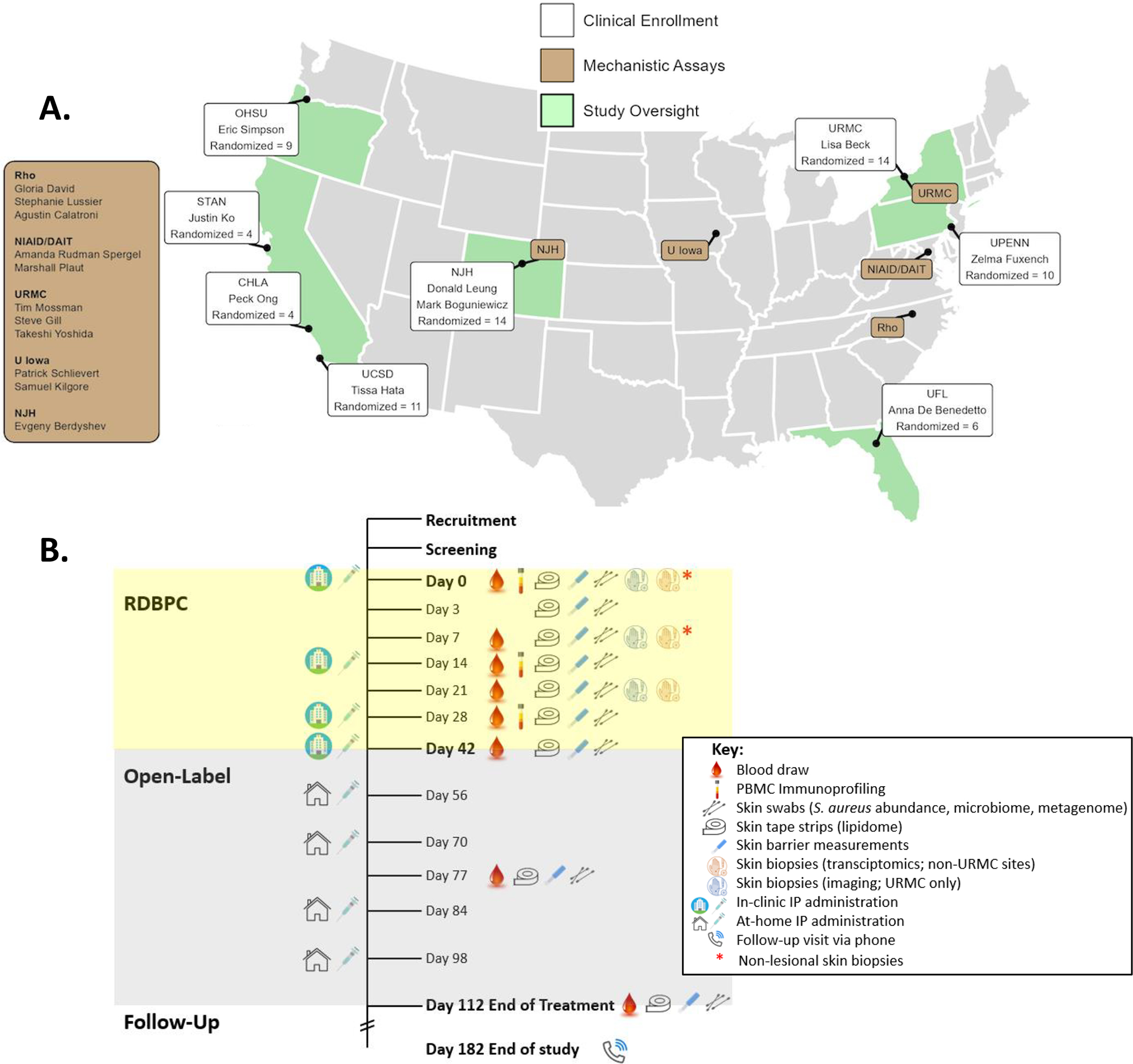
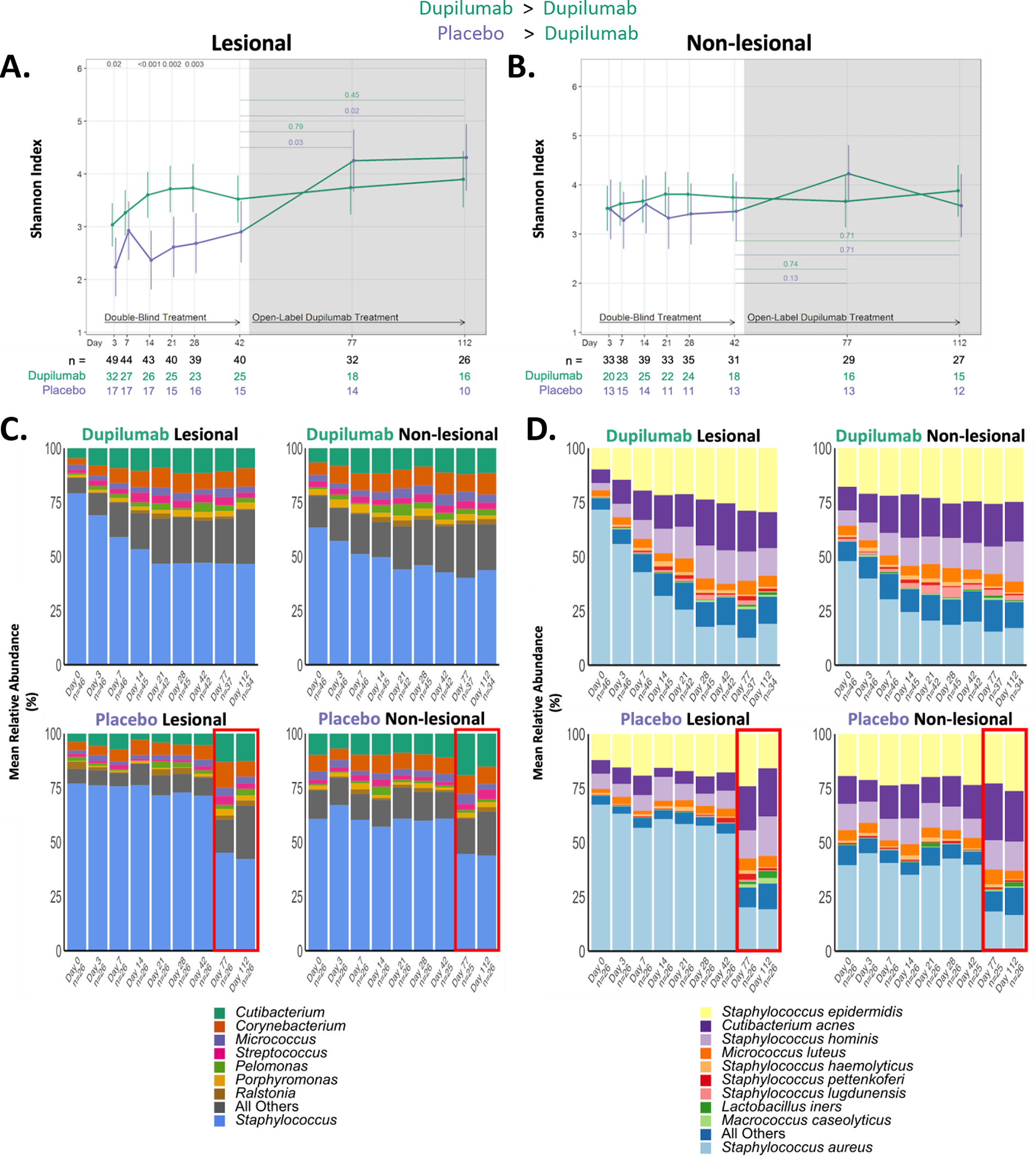
Methods: Participants (n = 71) with moderate-severe AD were enrolled in a randomized (dupilumab vs placebo; 2:1), double-blind study at Atopic Dermatitis Research Network centers. Bioassays were performed at multiple time points: S aureus and virulence factor quantification, 16s ribosomal RNA microbiome, serum biomarkers, skin transcriptomic analyses, and peripheral blood T-cell phenotyping.
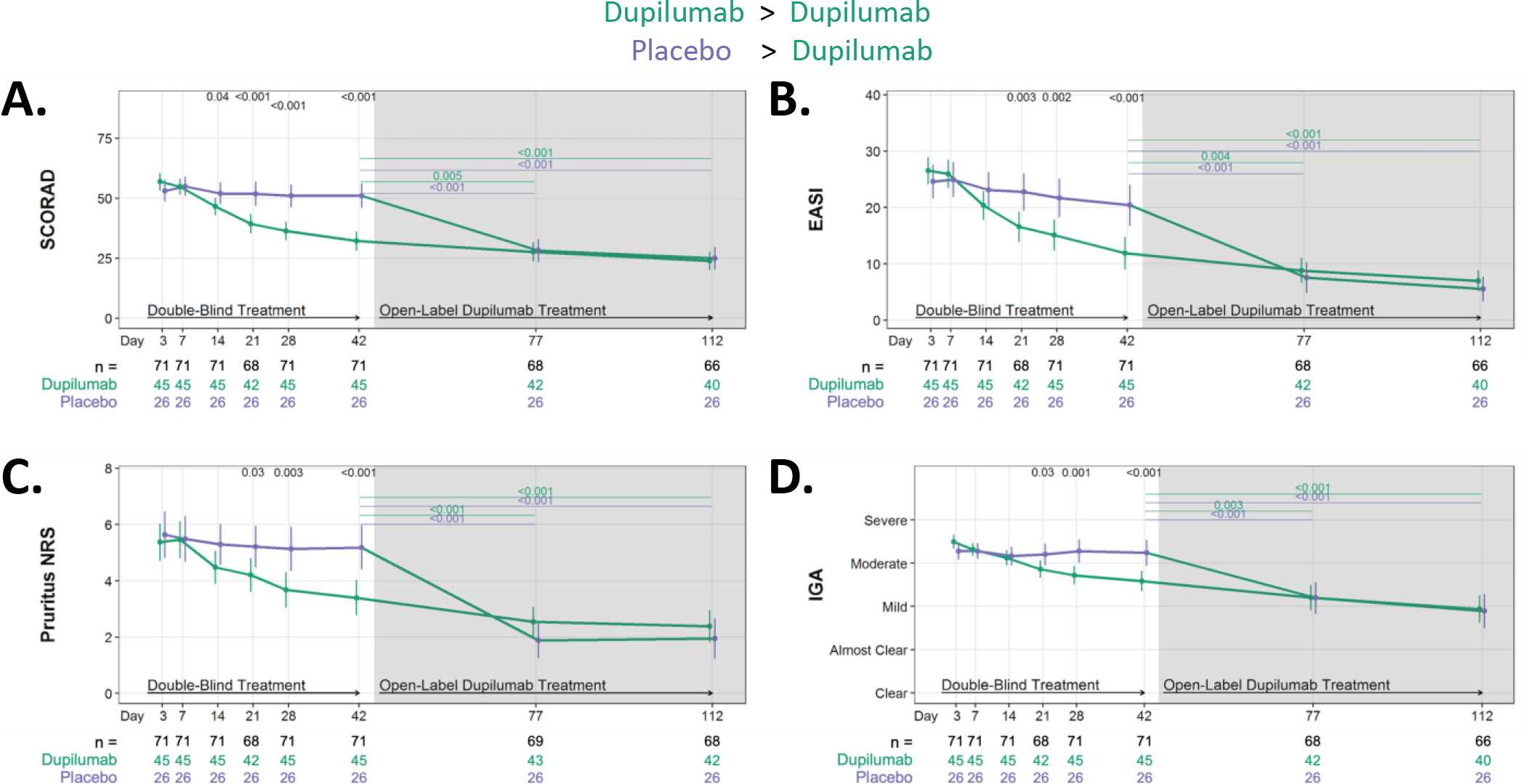
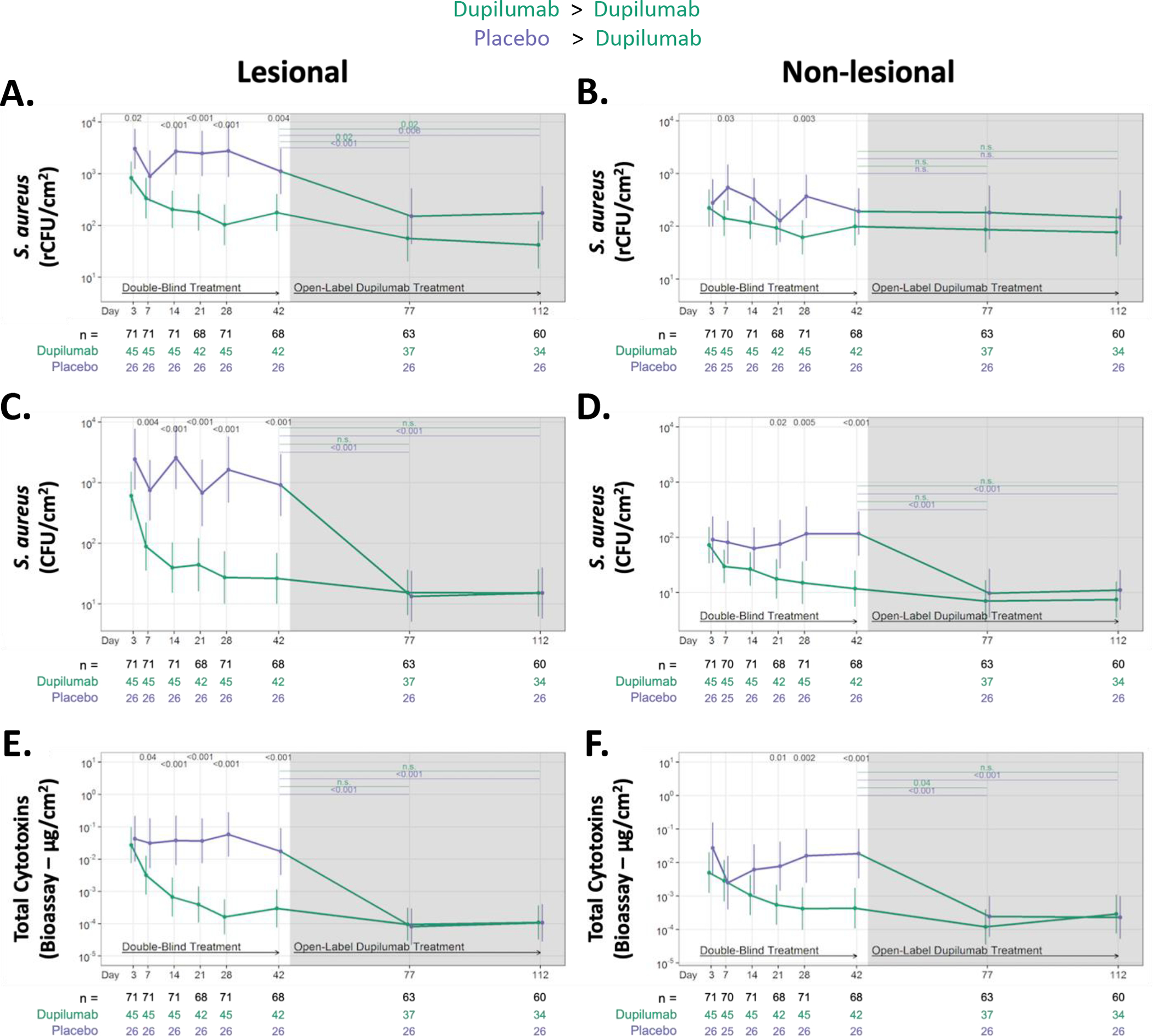
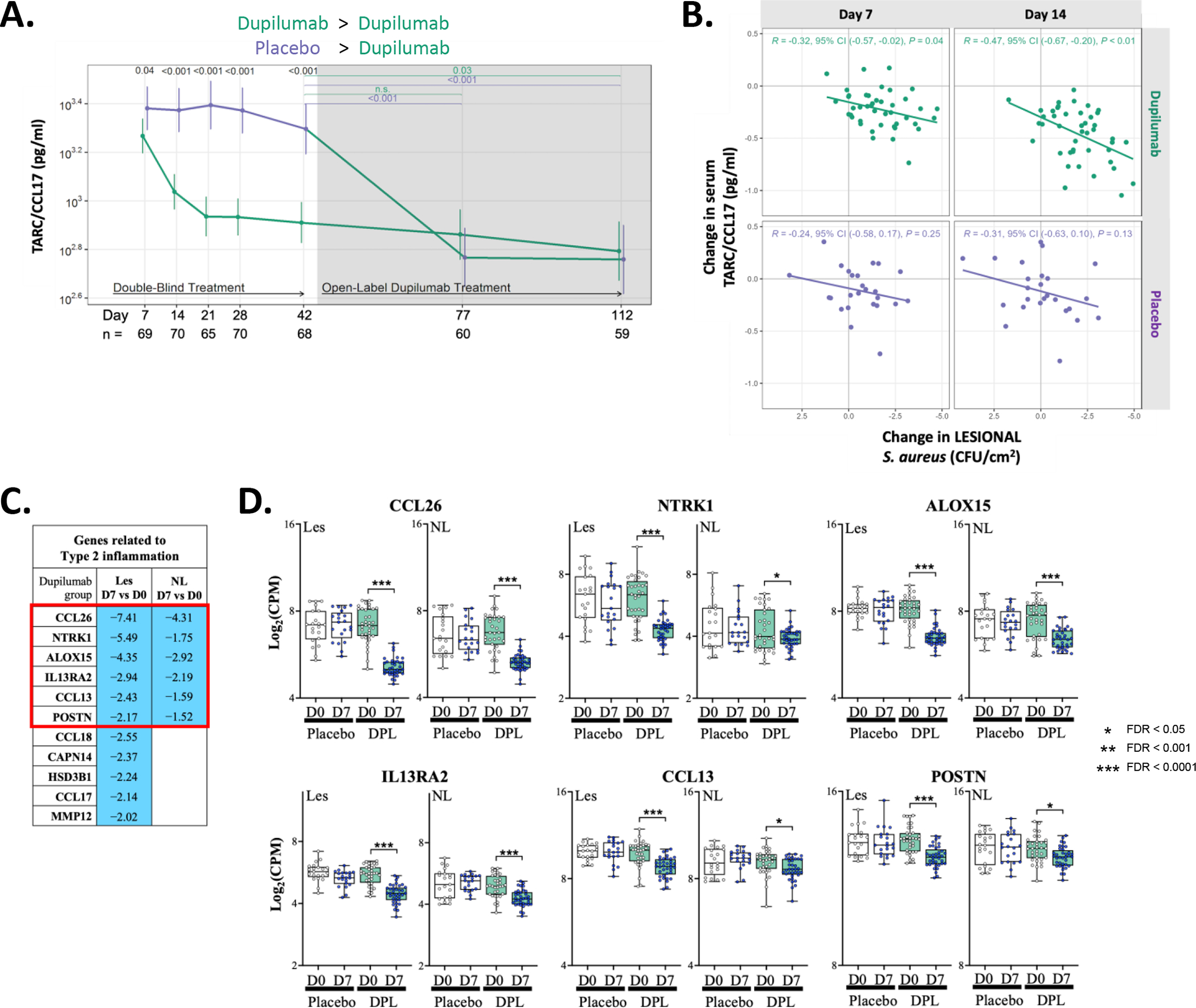
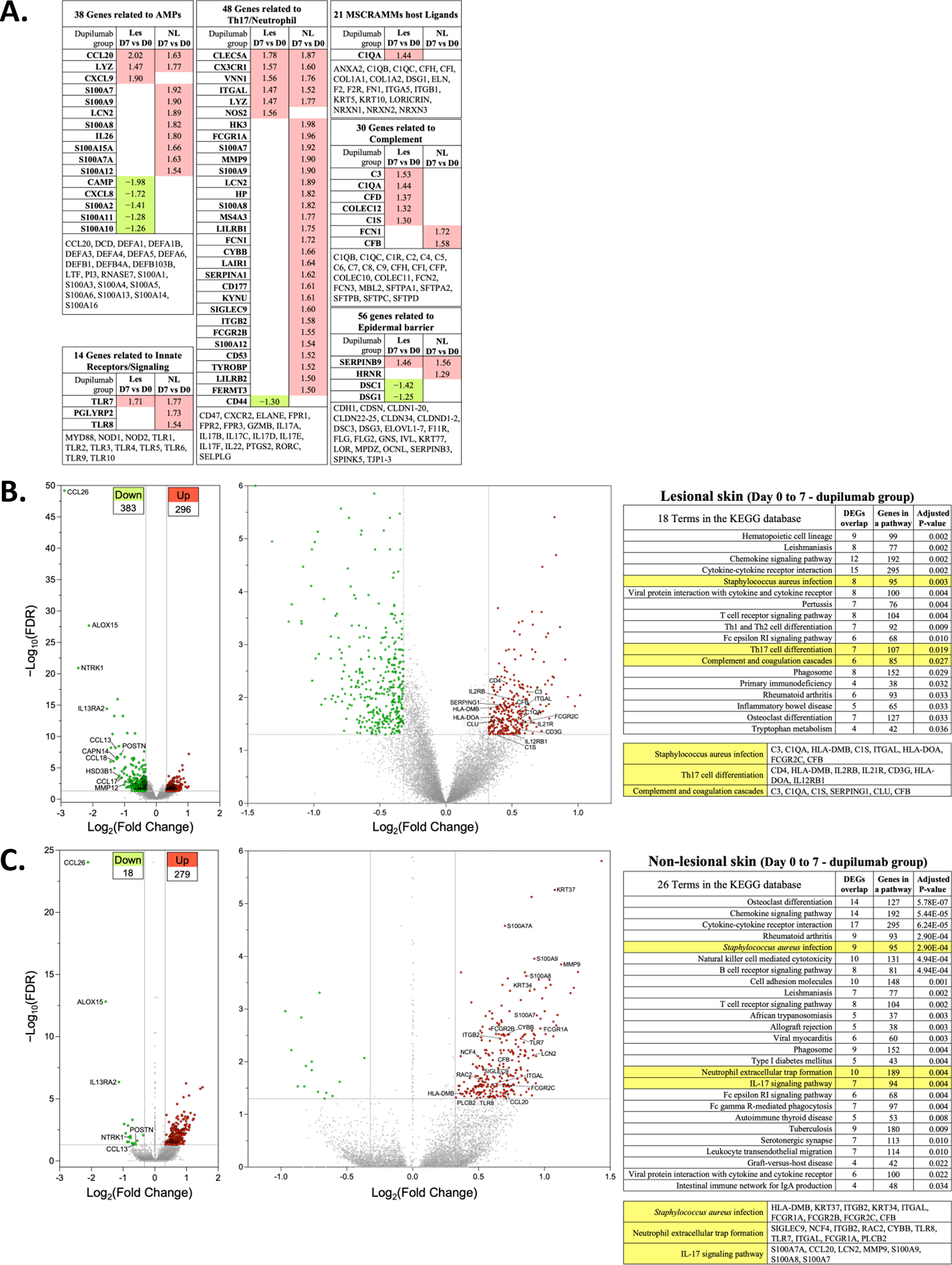
Results: At baseline, 100% of participants were S aureus colonized on the skin surface. Dupilumab treatment resulted in significant reductions in S aureus after only 3 days (compared to placebo), which was 11 days before clinical improvement. Participants with the greatest S aureus reductions had the best clinical outcomes, and these reductions correlated with reductions in serum CCL17 and disease severity. Reductions (10-fold) in S aureus cytotoxins (day 7), perturbations in TH17-cell subsets (day 14), and increased expression of genes relevant for IL-17, neutrophil, and complement pathways (day 7) were also observed.
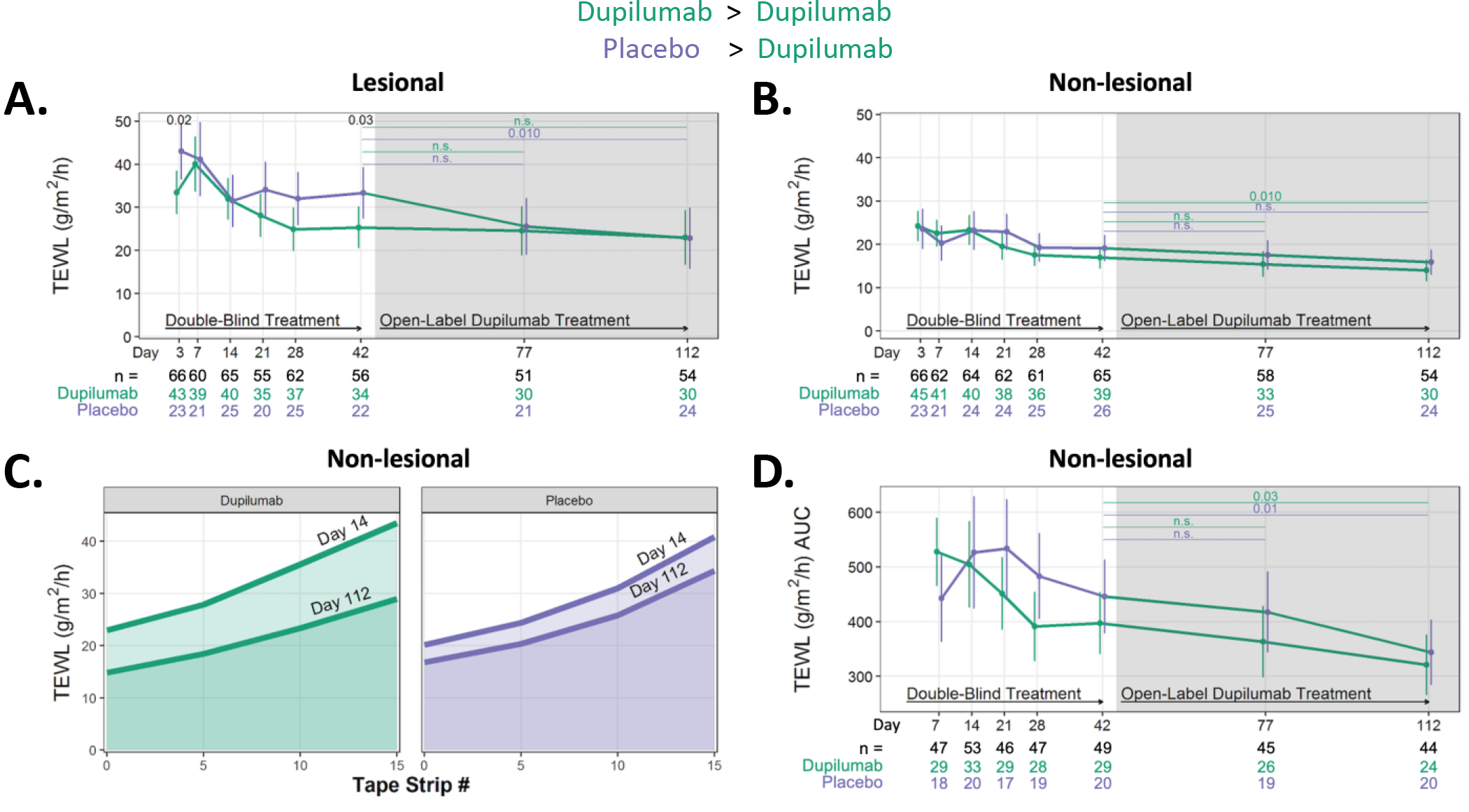
Conclusions: Blockade of IL-4 and IL-13 signaling, very rapidly (day 3) reduces S aureus abundance in subjects with AD, and this reduction correlates with reductions in the type 2 biomarker, CCL17, and measures of AD severity (excluding itch). Immunoprofiling and/or transcriptomics suggest a role for TH17 cells, neutrophils, and complement activation as potential mechanisms to explain these findings.
Keywords: Atopic dermatitis; IL-13; IL-17; IL-4; Staphylococcus aureus; barrier; cytotoxins; dupilumab; microbiome; type 2 immunity.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
