

Senescent cardiomyocytes contribute to cardiac dysfunction following myocardial infarction
- PMID: 37316516
- PMCID: PMC10267185
- DOI: 10.1038/s41514-023-00113-5
Senescent cardiomyocytes contribute to cardiac dysfunction following myocardial infarction
Erratum in
-
Author Correction: Senescent cardiomyocytes contribute to cardiac dysfunction following myocardial infarction.NPJ Aging. 2023 Jun 23;9(1):16. doi: 10.1038/s41514-023-00115-3. NPJ Aging. 2023. PMID: 37353486 Free PMC article. No abstract available.
Abstract
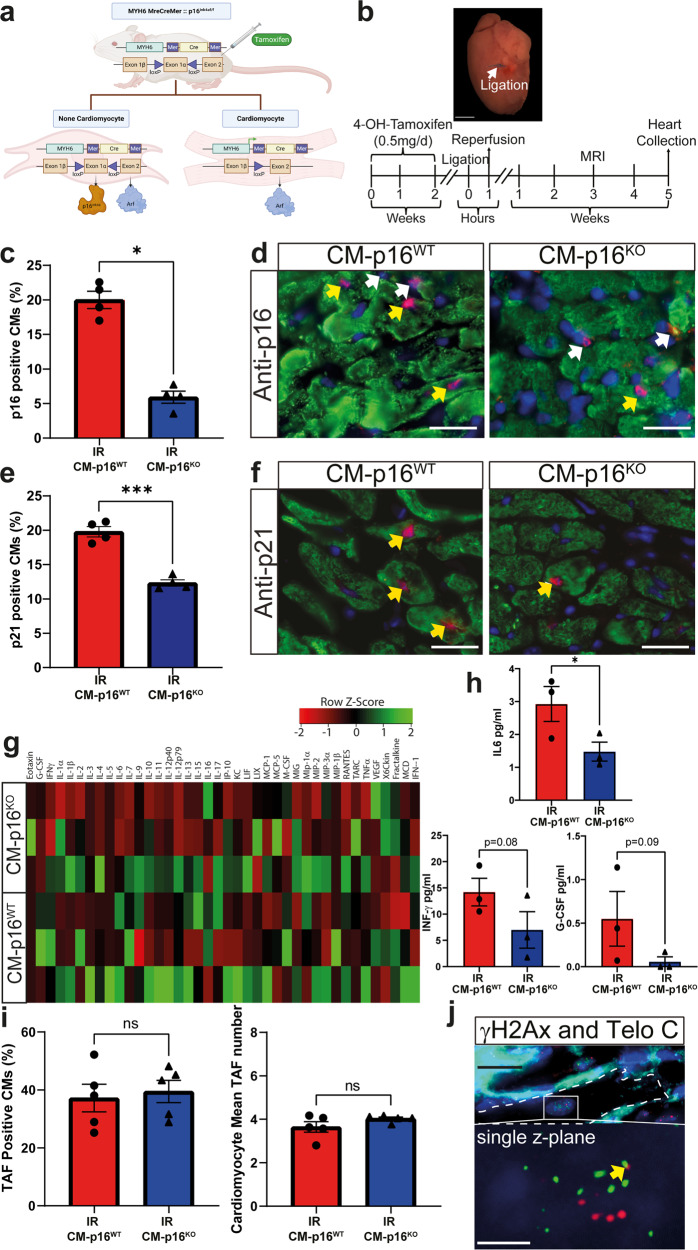
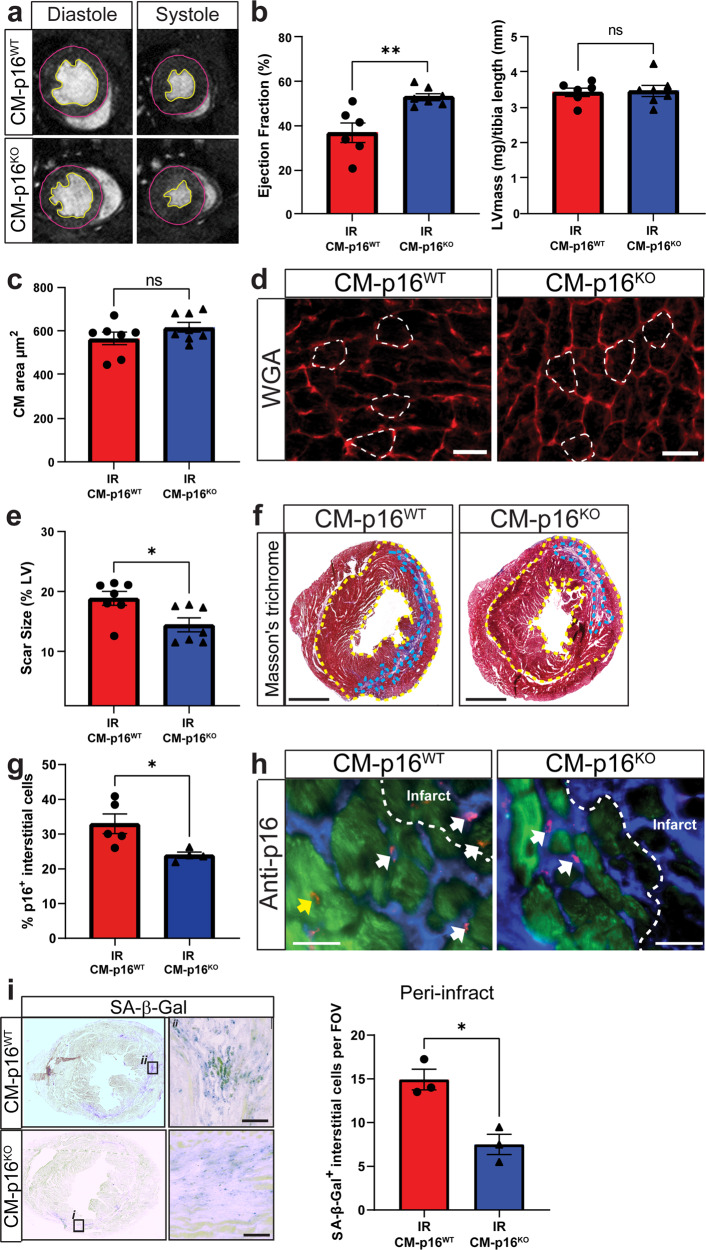
Myocardial infarction is a leading cause of morbidity and mortality. While reperfusion is now standard therapy, pathological remodelling leading to heart failure remains a clinical problem. Cellular senescence has been shown to contribute to disease pathophysiology and treatment with the senolytic navitoclax attenuates inflammation, reduces adverse myocardial remodelling and results in improved functional recovery. However, it remains unclear which senescent cell populations contribute to these processes. To identify whether senescent cardiomyocytes contribute to disease pathophysiology post-myocardial infarction, we established a transgenic model in which p16 (CDKN2A) expression was specifically knocked-out in the cardiomyocyte population. Following myocardial infarction, mice lacking cardiomyocyte p16 expression demonstrated no difference in cardiomyocyte hypertrophy but exhibited improved cardiac function and significantly reduced scar size in comparison to control animals. This data demonstrates that senescent cardiomyocytes participate in pathological myocardial remodelling. Importantly, inhibition of cardiomyocyte senescence led to reduced senescence-associated inflammation and decreased senescence-associated markers within other myocardial lineages, consistent with the hypothesis that cardiomyocytes promote pathological remodelling by spreading senescence to other cell-types. Collectively this study presents the demonstration that senescent cardiomyocytes are major contributors to myocardial remodelling and dysfunction following a myocardial infarction. Therefore, to maximise the potential for clinical translation, it is important to further understand the mechanisms underlying cardiomyocyte senescence and how to optimise senolytic strategies to target this cell lineage.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Senescent cardiomyocytes contribute to cardiac dysfunction following myocardial infarction.Res Sq [Preprint]. 2023 Apr 10:rs.3.rs-2776501. doi: 10.21203/rs.3.rs-2776501/v1. Res Sq. 2023. Update in: NPJ Aging. 2023 Jun 14;9(1):15. doi: 10.1038/s41514-023-00113-5. PMID: 37090497 Free PMC article. Updated. Preprint.
Similar articles
-
Senescent cardiomyocytes contribute to cardiac dysfunction following myocardial infarction.Res Sq [Preprint]. 2023 Apr 10:rs.3.rs-2776501. doi: 10.21203/rs.3.rs-2776501/v1. Res Sq. 2023. Update in: NPJ Aging. 2023 Jun 14;9(1):15. doi: 10.1038/s41514-023-00113-5. PMID: 37090497 Free PMC article. Updated. Preprint.
-
Pharmacological clearance of senescent cells improves survival and recovery in aged mice following acute myocardial infarction.Aging Cell. 2019 Jun;18(3):e12945. doi: 10.1111/acel.12945. Epub 2019 Mar 28. Aging Cell. 2019. PMID: 30920115 Free PMC article.
-
Cardiomyocyte senescence and the potential therapeutic role of senolytics in the heart.J Cardiovasc Aging. 2024 Apr;4(2):18. doi: 10.20517/jca.2024.06. Epub 2024 May 30. J Cardiovasc Aging. 2024. PMID: 39119147 Free PMC article.
-
Cardiomyocyte Senescence and Cellular Communications Within Myocardial Microenvironments.Front Endocrinol (Lausanne). 2020 May 21;11:280. doi: 10.3389/fendo.2020.00280. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32508749 Free PMC article. Review.
-
Cardiomyocytes Cellular Phenotypes After Myocardial Infarction.Front Cardiovasc Med. 2021 Nov 8;8:750510. doi: 10.3389/fcvm.2021.750510. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34820429 Free PMC article. Review.
Cited by
-
Anti-senescence therapies: a new concept to address cardiovascular disease.Cardiovasc Res. 2025 May 23;121(5):730-747. doi: 10.1093/cvr/cvaf030. Cardiovasc Res. 2025. PMID: 40036821 Free PMC article. Review.
-
SPaSE: Spatially resolved pathology scores using optimal transport on spatial transcriptomics data.Cell Syst. 2025 Jul 16;16(7):101301. doi: 10.1016/j.cels.2025.101301. Epub 2025 Jun 5. Cell Syst. 2025. PMID: 40480226
-
Geroscience in heart failure: the search for therapeutic targets in the shared pathobiology of human aging and heart failure.J Cardiovasc Aging. 2025;5(1):10.20517/jca.2024.15. doi: 10.20517/jca.2024.15. Epub 2025 Jan 14. J Cardiovasc Aging. 2025. PMID: 40297496 Free PMC article.
-
Interplay between Senescence and Macrophages in Diabetic Cardiomyopathy: A Review of the Potential Role of GDF-15 and Klotho.Biomedicines. 2024 Mar 29;12(4):759. doi: 10.3390/biomedicines12040759. Biomedicines. 2024. PMID: 38672115 Free PMC article. Review.
-
Injury minimization after myocardial infarction: focus on extracellular vesicles.Eur Heart J. 2024 May 13;45(18):1602-1609. doi: 10.1093/eurheartj/ehae089. Eur Heart J. 2024. PMID: 38366191 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
