

Functional connectivity discriminates epileptogenic states and predicts surgical outcome in children with drug resistant epilepsy
- PMID: 37316544
- PMCID: PMC10267141
- DOI: 10.1038/s41598-023-36551-0
Functional connectivity discriminates epileptogenic states and predicts surgical outcome in children with drug resistant epilepsy
Abstract
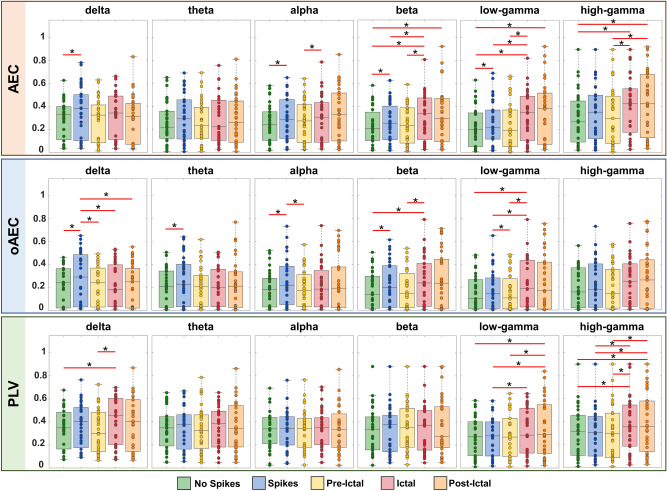
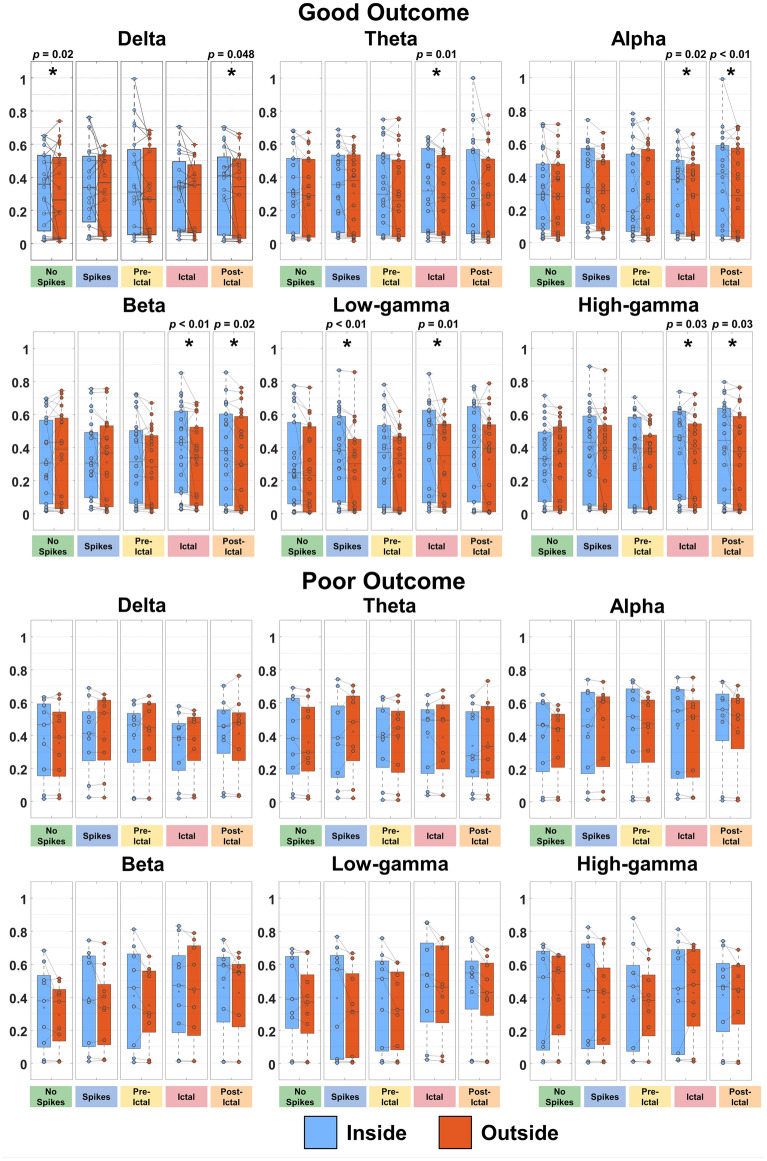
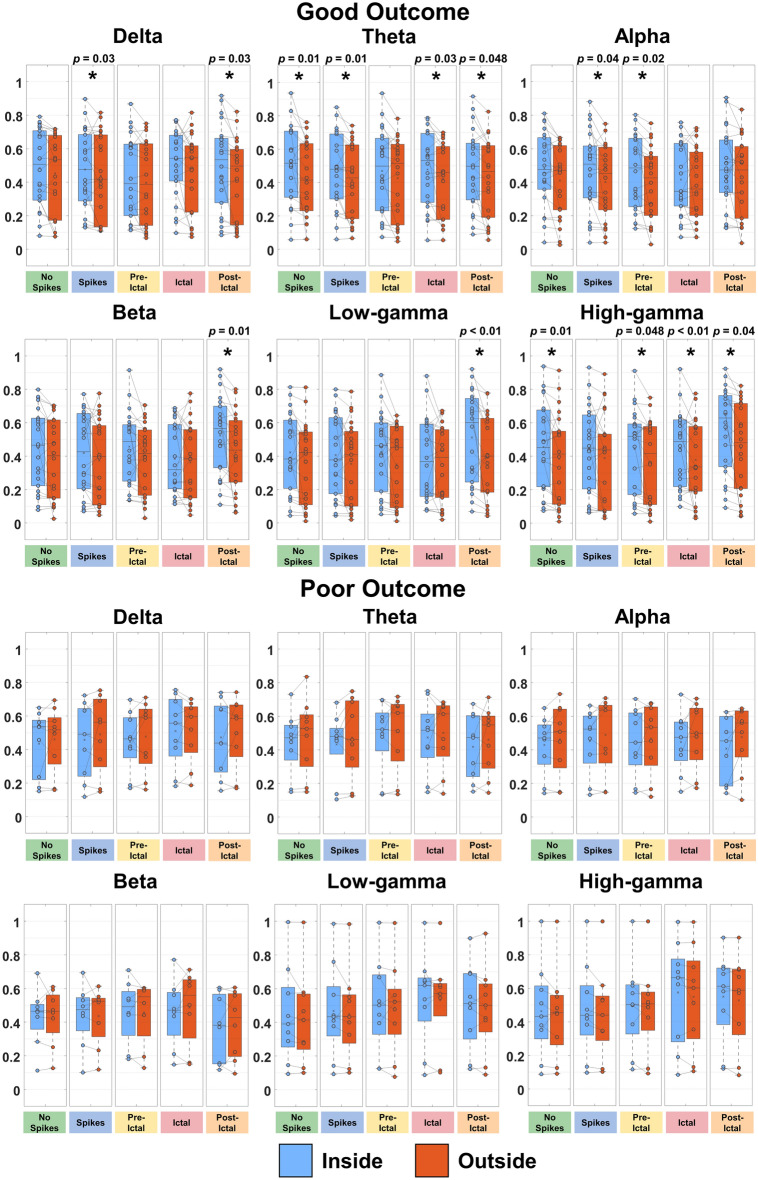
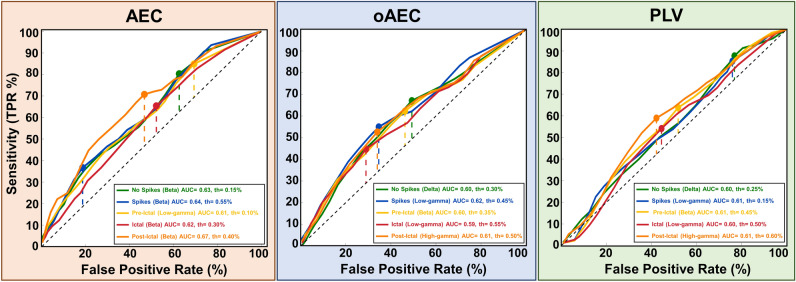
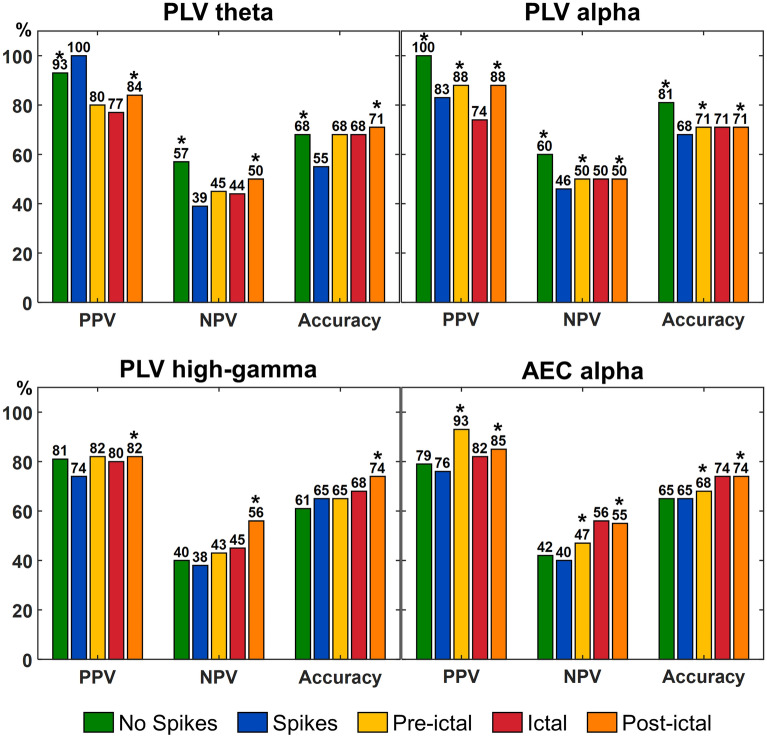
Normal brain functioning emerges from a complex interplay among regions forming networks. In epilepsy, these networks are disrupted causing seizures. Highly connected nodes in these networks are epilepsy surgery targets. Here, we assess whether functional connectivity (FC) using intracranial electroencephalography can quantify brain regions epileptogenicity and predict surgical outcome in children with drug resistant epilepsy (DRE). We computed FC between electrodes on different states (i.e. interictal without spikes, interictal with spikes, pre-ictal, ictal, and post-ictal) and frequency bands. We then estimated the electrodes' nodal strength. We compared nodal strength between states, inside and outside resection for good- (n = 22, Engel I) and poor-outcome (n = 9, Engel II-IV) patients, respectively, and tested their utility to predict the epileptogenic zone and outcome. We observed a hierarchical epileptogenic organization among states for nodal strength: lower FC during interictal and pre-ictal states followed by higher FC during ictal and post-ictal states (p < 0.05). We further observed higher FC inside resection (p < 0.05) for good-outcome patients on different states and bands, and no differences for poor-outcome patients. Resection of nodes with high FC was predictive of outcome (positive and negative predictive values: 47-100%). Our findings suggest that FC can discriminate epileptogenic states and predict outcome in patients with DRE.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
